PORTAL VENOUS SYSTEM
Portal Vein
The portal vein is about 7 to 8 cm in length and carries the visceral blood to the liver,
where it ramifies following the segmental pattern,
reaching the sinusoids,
from which the blood again converges to drain into the inferior vena cava through the hepatic veins.
The portal vein results from the confluence of the splenic vein and the superior mesenteric vein.
Besides the splenic and the superior mesenteric veins,
other tributaries are the left gastric,
right gastric,
the paraumbilical,
and cystic veins.
Splenic Vein
The splenic vein is one of the two larger tributaries of the portal vein,
and its confluence with the superior mesenteric vein actually forms the portal vein.
Tributaries: short gastric veins,
left gastroepiploic vein,
pancreatic vein.
Inferior Mesenteric Vein
The inferior mesenteric vein drains the rectum,
the sigmoid colon and the left colon,
joining the splenic vein distally,
close to the confluence with the inferior mesenteric vein.
Occasionally it ends at the union of the splenic and superior mesenteric vein,
and sometimes at the superior mesenteric vein itself.
Tributaries,
superior rectal vein,
sigmoid veins,
left colic vein.
Superior Mesenteric Vein
The superior mesenteric vein is the largest tributary to the portal vein.
It drains the small intestine,
cecum,
and ascending and transverse parts of the colon,
carrying the blood to enter the portal circulation.
The superior mesenteric vein is formed by the union of the tributaries from the terminal ileum,
the cecum,
and the appendix,
receiving several other tributaries along its length.
ANASTOMOSES BETWWEN THE PORTAL AND SYSTEMIC CIRCULATION
In portal vein obstruction or portal vein hypertension due to liver disease,
anastomoses between the portal vein and systemic veins may develop,
carrying portal blood into the systemic circulation[3].
There are four main groups of portal systemic collaterals.
Group I - protective mucosal epithelium adjoins absorptive epithelium.
Group I (A) At the cardia of the stomach,
where the left gastric vein and short gastric veins of the portal system anastomoses with the intercostal,
diaphragm–esophageal,
and azygos tributaries,
veins of the caval system,
creating esophageal and gastric fundus varices.
Group I (B) At the anal canal the superior rectal (hemorrhoidal) vein,
tributary of the inferior mesenteric vein (portal system),
anastomoses with the middle and inferior rectal (hemorrhoidal) veins of the inferior vena cava system,
creating hemorrhoids.
Group II - In the falciform ligament through the paraumbilical veins,
vestiges of the umbilical circulation of fetal life.
The enlargement of these connections,
in the presence of portal hypertension,
may produce varices of veins radiating from the umbilicus,
the caput medusae (part of the Cruveilhier-Baumgarten syndrome).
The remaining umbilical vein does not rechannel within the ligamentum teres.
Group III - the abdominal organs are in contact with retroperitoneal tissues or adherent to the abdominal wall (intercostal veins,
lumbar veins).
Includes veins from the liver to the diaphragm (veins of Sappey),
veins in the lienorenal ligament and omentum,
lumbar veins (veins of Retzius),
and veins developed in adhesions and scars of previous surgeries.
Group IV - Connections between the portal system and the left renal vein.
This may be through communications directly from the splenic vein or via diaphragmatic,
pancreatic,
left adrenal,
gonadal,
or gastric veins.
Other Collaterals
The communications from the gastroesophageal collaterals,
retroperitoneal,
and venous systems of the abdomen eventually reach the superior vena cava via the azygos or hemiazygos systems.
Very rarely a patent ductus venosus connects the left branch of the portal vein to the inferior vena cava.
In cases of extrahepatic portal venous obstruction,
additional collaterals develop toward the liver,
entering the liver through the portal vein in the porta hepatis.
These collaterals include the veins at the hilum,
venae comitantes of the portal vein and hepatic arteries,
veins in the suspensory ligaments of the liver,
unnamed veins around the gallbladder,
and diaphragmatic and omental veins.
Spontaneous portosystemic shunts (Fig.
1)
1. connection to superior vena cava
- esophageal varices (between subepithelial and submucosal veins) supplied by anterior branch of left gastric vein
- paraesofageal varices supplied by posterior branch of coronary (left gastric) vein draining into azygos and hemiazygos venules and vertebral plexus.
They are not connected to esophageal varices
2 connection to pulmonary circulation
- gastropulmonary shunt (between gastric or esophageal vein and left pericardiophrenic or inferior pulmonary veins)
3 retrograde mesenteric flow
- veins of Retzius (anastomoses between portal vein and inferior vena cava)
ileocolic veins – right gonadal vein – IVC
pancreaticoduodenal vein – IVC
proximal small left branches of superior mesenteric vein – left gonadal vein – left renal vein
ileocolic veins – directly into IVC
4 retroperitoneal collaterals
- splenorenal or splenoadrenorenal shunts
- gastrorenal shunt
- mesenterorenal shunt (between superior mesenteric vein and right renal vein)
- mesenterogonadal shunt (between ileocoloc vein and right testicular vein)
- splenocaval shunt (between splenic vein and left hypogastric vein)
5 intrahepatic shunt (portal vein to hepatic vein)
6 Cruveilhier-von Baumgarten syndrome
|
Spontaneous portosystemic Shunts
|
|
Type of varices
|
Frequency (%)
|
|
Coronary venous
|
80-86
|
|
Esophageal
|
45-65
|
|
Paraumbilical
|
10-43
|
|
Abdominal wall
|
30
|
|
Perisplenic
|
30
|
|
Retrogastric/gastric
|
2-27
|
|
Paraesophageal
|
22
|
|
Omental
|
20
|
|
Retroperitoneal-paravertebral
|
18
|
|
Mesenteric
|
10
|
|
Splenorenal
|
10
|
|
Gastrorenal
|
7
|
CT APPEARANCES OF VARICES IN PORTAL HIPERTENSION
On CT scan varices appear as well defined,
round,
tubular,
or serpentine structures,
that are smooth,
have homogeneous attenuation,
and enhance with contrast material to the same degree as adjacent vessels [4].
Varices are usually easy to detect on CT scan because are often surrounded by the fat in retroperitoneum,
greater or lesser omentum and mesentery.
Because without contrast they mimic pathological masses as adenopathy or tumors as well as bowel loops it is necessary to inject contrast.
Coronary venous collateral vessels
Are the most common seen portosystemic collaterals pathways in portal hypertension with a frequency of 80-86%.
They are the most important collateral in cranially directed hepatofugal flow.
Coronary and short gastric venous collaterals are usually drained via coexisting esophageal and paresophageal varices and occasionally via spontaneous gastrorenal or splenorenal shunts.
These appear as vascular channels in the triangular fatty tissue between the medial wall of upper gastric body and posterior margin of left hepatic lobe,
the lesser omentum.
(Fig.
2)

Fig.: Dilated vessels in the triangular fatty tissue between the medial wall of upper gastric body and posterior margin of left hepatic lobe (black arrows).
References: Arcadia Medical Center, Iasi / Romania 2010
A left gastric vein larger than 5-6 mm or multiple dilated veins 4-6 mm in diameter in the lesser omentum on CT scan is considered abnormal and is an indicator in portal hypertension [4].
(Fig.
3).
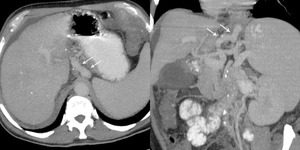
Fig.: Patient with cirrhosis and portal hypertension.
Dilated coronary vein (white arrows)
References: Arcadia Medical Center, Iasi / Romania
Usually,
coronary venous collaterals are asociated with esophageal and paraesophageal varices and occasionally can associate retrogastric varices.
Gastric varices
Fed by left gastric vein or gastroepiploic vein gastric varices drain via esophageal or parasophageal veins and further into azygos or hemiazygos vein system.
They appearance on CT scan as multiple round or tubular areas of increased attenuation in the posterior or postero-medial aspect of gastric fundus,
near the cardia[4].
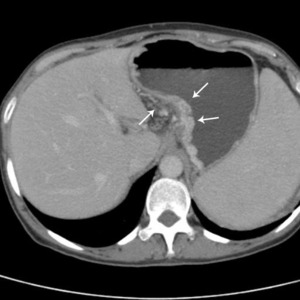
Fig.: Dilated submucosal veins prominent in gastric lumen, near the cardia (arrows).
References: Arcadia Medical Center, Iasi / Romania 2010
Esophageal and paraesophageal varices
Esophageal varices are the most common source of gastrointestinal hemorrhage.
Esophageal varices are formed by dilated subepithelial and submucosal vein and the dilated accompanying veins of vagus nerves that lie in the adventitia outside of tunica muscularis and are usually supplied by the anterior branch of the left gastric vein.
The size of the varices depends on the degree of portal hypertension and the presence of other portosystemic collaterals.[5]
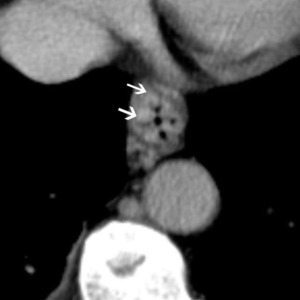
Fig.: The CT appearances of esophageal varices are as intraluminal protrusion with scalloped margins (arrows).
References: Arcadia Medical Center, Iasi / Romania 2010
Paraesophageal varices are collateral vessels in the posterior mediastinum beyond the esophageal wall,
supplied by posterior branch of left gastric vein draining into azygos and hemiazygos venules and vertebral plexus.
They are situated outside the wall of the esophagus in the mediastinum,
parallel with the esophageal veins at the distance of 1-2 cm without direct communication with them.
They are not connected to esophageal varices.
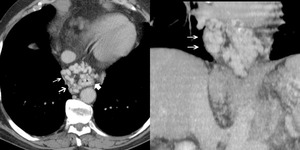
Fig.: Paraesophageal varices (white double arrows) appear as well defined, round, tubular, or serpentine structures situated outside the wall of the esophagus in the mediastinum.
References: Arcadia Medical Center, Iasi / Romania 2010
Endoscopy is the most reliable diagnostic procedure for detecting oesophageal varices.
CT is able to detect paraesophageal varices and esophageal collateral vessels.
Paraumbilical venous collateral vessels and abdominal wall varices
The normal falciform ligament contains 1-3 paraumbilical veins.
They are normally tiny and collapsed,
and due to portal hypertension the number and caliber of this vein increase.
They arise from left portal vein and accompany the falciform ligament downwards to the umbilicus.
On CT scans they appear as nodular or serpentine enhancing structures usually more than 3 mm diameter.

Fig.: Dilated paraumbilical veins anterior to left hepatic lobe (black arrows) arising from left portal vein (white arrow).
References: Arcadia Medical Center, Iasi / Romania 2010
Abdominal wall varices appear as prominent veins radiating from the umbilicus.
Usually they are one or two.
When they are in large number the condition are named caput medusae,
but this is rare.
These collaterals are connected with superior and inferior epigastric veins and are fed by the paraumbilical and omental veins.
The vast majority of paraumbilical flow return to the systemic circulation via one of the inferior epigastric vein (Fig 8).

Fig.: Abdominal wall varices radiating from the umbilicus. Connection with superior epigastric veins (A and C) inferior epigastric veins (D) and multiple vessels forming caput medusae (B).
References: Arcadia Medical Center, Iasi / Romania 2010
The abdominal wall varices are easily identified on CT scans because they are surrounded by fatty subcutaneous tissue.
Perisplenic varices
They appear as dilated veins antero-inferior to the spleen or superiorly and posteriory and may extend to the left kidney.
May communicate with retrogastric varices or dilated inferior frenic veins (Fig.
9).
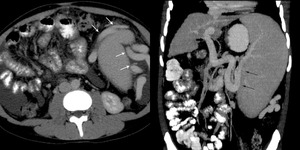
Fig.: Large perisplenic varices (white arrows) and dilated splenic vein (black arrows).
References: Arcadia Medical Center, Iasi / Romania 2010
Mesenteric varices
Appear as dilated or tortuous branches of mesenteric vein in the depth of mesentery.
These varices communicate with systemic veins via the retro-peritoneal and mesenteric venous plexus (Fig.
10)

Fig.: Multiple round areas of increased attenuation in the depth of mesentery.
References: Arcadia Medical Center, Iasi / Romania 2010
Omental varices
The CT appearances of omental varices are as numerous tortuous areas of increased attenuation in the greater omentum (Fig.11).
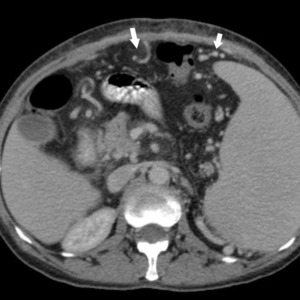
Fig.: Dilated vessels in the great omentum (white arrows)
References: Arcadia Medical Center, Iasi / Romania 2010
Splenorenal or splenoadrenorenal shunts
Are seen as large,
tortuous veins between splenic and left renal hilus that drain into left renal vein and further into inferior vena cava. They can decompress the high pressure portal flow and produce a low portosystemic pressure gradient (Fig.
12).
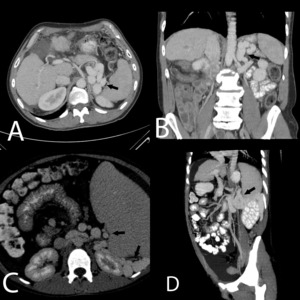
Fig.: Direct spleno-renal shunt (A and B) and indirect shunt via perisplenic and left perirenal space vessels (C and D).
References: Arcadia Medical Center, Iasi / Romania 2010
Transhepatic portosystemic shunts
Transhepatic portosystemic shunts are classified as two types on the basis of the draining vein:
- in the hepatic venous type,
the intrahepatic portal vein communicates with the hepatic vein in or on the surface of the liver (Fig.
13).
- in the systemic venous type,
the intrahepatic portal vein runs toward the outside of the liver and communicates with the systemic veins (Fig.
14).
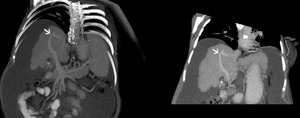
Fig.: Intrahepatic portosystemic shunt between anterior branch of portal vein and right hepatic vein afluent (white arrow)
References: Arcadia Medical Center, Iasi/Romania 2010
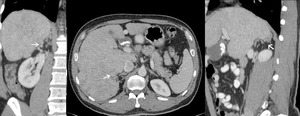
Fig.: Branch of intrahepatic right portal vein communicates via perirenal collaterals with right renal vein and drains the portal flow into inferior vena cava.
References: Arcadia Medical Center, Iasi / Romania 2010
Venous collaterals between inferior mesenteric vein and inferior vena cava (Fig.
15.
It is possible to have a direct connection through multiple collaterals that divert portal flow between inferior mesenteric vein and inferior vena cava.

Fig.: Dilated round vessels (arrows) joining inferior mesenteric vein with inferior vena cava.
References: Arcadia Medical Center, Iasi / Romania 2010
Anal canal varices
At the anal canal the superior rectal (hemorrhoidal) vein,
tributary of the inferior mesenteric vein (portal system),
anastomoses with the middle and inferior rectal (hemorrhoidal) veins of the inferior vena cava system,
creating hemorrhoids (Fig.
16).
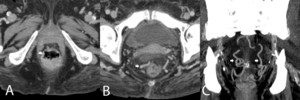
Fig.: Internal hemorrhoids (A)and perirectal venous collateral circulation (B and C).
References: Arcadia Medical Centre, Iasi / Romania 2010


. References: Arcadia Medical Center, Iasi / Romania 2010")
 References: Arcadia Medical Center, Iasi / Romania")
. References: Arcadia Medical Center, Iasi / Romania 2010")
. References: Arcadia Medical Center, Iasi / Romania 2010")
 appear as well defined, round, tubular, or serpentine structures situated outside the wall of the esophagus in the mediastinum. References: Arcadia Medical Center, Iasi / Romania 2010")
 arising from left portal vein (white arrow). References: Arcadia Medical Center, Iasi / Romania 2010")
 inferior epigastric veins (D) and multiple vessels forming caput medusae (B). References: Arcadia Medical Center, Iasi / Romania 2010")
 and dilated splenic vein (black arrows). References: Arcadia Medical Center, Iasi / Romania 2010")

 References: Arcadia Medical Center, Iasi / Romania 2010")
 and indirect shunt via perisplenic and left perirenal space vessels (C and D). References: Arcadia Medical Center, Iasi / Romania 2010")
 References: Arcadia Medical Center, Iasi/Romania 2010")

 joining inferior mesenteric vein with inferior vena cava. References: Arcadia Medical Center, Iasi / Romania 2010")
and perirectal venous collateral circulation (B and C). References: Arcadia Medical Centre, Iasi / Romania 2010")