Type:
Educational Exhibit
Keywords:
Neuroradiology brain, Interventional vascular, Vascular, Catheter arteriography, Fluoroscopy, MR, Angioplasty, Stents, Catheters, Arteriovenous malformations, Aneurysms, Embolism / Thrombosis
Authors:
D. Ruijters, R. Homan, P. Mielekamp, D. Babic; Best/NL
DOI:
10.1594/ecr2012/C-1183
Imaging findings OR Procedure details
Workflow
- The pre-procedural multi-modal data in DICOM format is imported into the interventional workstation from a PACS or disc.
- Peri-interventionally,
a cone-beam CT (optionally contrast enhanced) is acquired with the C-arm system,
see movie below.

Fig. 6: Rotational cone-beam CT acquisition.
References: Ruijters D et al. (2009) Real-time integration of 3-D multimodality data in interventional neuroangiography. J Electron Imaging 18(3)
- The cone-beam CT is co-registered with the multi-modal data,
using a semi-automatic approach,
by selecting the overlay tool on the 3D workstation.
A coarse manual initialization in axial,
coronal and sagittal viewing direction is performed by the operator.
Then the fine co-registration can be performed by the software,
see movie below.
Finally,
the co-registration result is to be visually inspected by the operator.
Fig. 7: Fast automatic MR - CT-conebeam co-registration.
References: Ruijters D et al. (2009) Real-time integration of 3-D multimodality data in interventional neuroangiography. J Electron Imaging 18(3)
- The 3D roadmapping is activated by pressing the "3D Roadmap" button on the table side touch screen module.
There are several visualization options that can be chosen by the operator.
The multi-modal data can be either visualized as a oblique slab that is always oriented parallel with viewport,
see figure below.
It is important to place the center of rotation within the lesion.
In that way,
the lesion stays within the rotated oblique slab when the gantry is rotated.
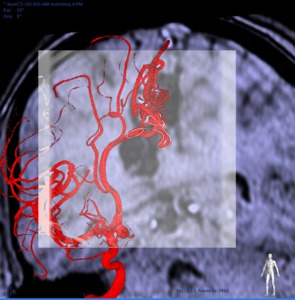
Fig. 5: MR Roadmap.
References: Ruijters D et al. (2011) Validation of 3D multimodality roadmapping. Phys. Med. Biol. 56:5335-54
Alternatively, the multi-modal data can be shown in volume render mode,
see movie below.
The cone-beam CT can then optionally be hidden.
In that case the cone-beam CT is used for co-registration purposes only.
Fig. 8: CTA Roadmap, showing real-time compensation for table movements.
References: Courtesy of Dr. Maleux, UZ Leuven, Belgium
Accuracy
The accuracy of the automatic multimodal registration algorithm was validated using a head phantom to deliver a ground truth [4].
On average an absolute residual translation error of 0.515 mm (std = 0.017,
min = 0.495,
max = 0.588) and a mean absolute residual rotation error of 0.241 degrees (std = 0.031,
min = 0.180,
max = 0.307) was obtained,
which corresponded to sub-voxel accuracy.
During the roadmapping phase the projection of the cone-beam CT dataset on fluoroscopy can be performed very accurately; The average deviation of the detector center amounts to about 0.1 mm in-plane,
the displacement of the focal spot is about 0.17 mm and the average rotational error is less than 0.1 degrees [4].
Analogous to the advice of Fahrig and Holdsworth [5],
the clinical systems are recalibrated every 6 months.
