There are 2 kinds of hearing loss,
conductive and/or sensorineural.
Some diseases that cause hearing loss demonstrate normal radiologic findings,
for example,
stapes footplate fixation,
sudden deafness,
senile deafness,
acoustic trauma,
and psychogenic deafness; others can be diagnosed by CT/MRI.
Radiologists should be familiar with the imaging features of these diseases.
We review the main diseases that can be diagnosed by CT/MRI and present those imaging findings.
Conductive or mixed hearing loss

Fig. 6: Flow chart for diagnosing conductive or mixed hearing loss with CT
♣Chronic otitis media
Chronic otitis media (COM) lasts 3 months or more.
Most cases do not require imaging diagnosis,
but CT assessment is useful when complications,
such as coalescent mastoiditis,
labyrinthitis,
or tympanosclerosis,
are suspected.
In patients with COM,
severe conductive deafness,
repeated ear discharge,
and coalescent mastoiditis are indications for surgical treatment,
including myringoplasty and mastoidectomy.
♣Attic (pars flaccida) cholesteatoma
Attic cholesteatomas comprise 80% or fewer of acquired-type cholesteatomas.
When pressure in the attic causes the cranial portion of the tympanum above the upper wall of the external auditory canal to become negative as a result of ventilatory insufficiency caused by auditory tube dysfunction,
a retraction pocket can easily form on the flaccid membrane.
The pocket often expands with continuous ventilatory insufficiency in the tympanum,
and cholesteatoma occurs as debris accumulates in the pocket.
CT shows soft tissue in the Prussak’s space (lateral epitympanic recess),
which is located between the attic lateral wall and malleus head,
as well as erosion of the scutum,
internal displacement of the ossicles,
and destruction of the ossicular chain.
Furthermore,
advanced cholesteatoma can destroy the facial nerve canal,
semicircular canals,
or cochlea.
No staging system for cholesteatoma has been universally adapted.
We introduce a system and treatment choices proposed by Yanagihara and Hinohira.
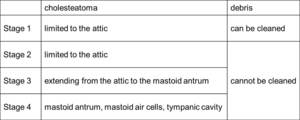
Table 1: Sample staging system for cholesteatoma

Fig. 7: Illustration of staging system for cholesteatoma
(a) Stage 1: The cholesteatoma (black area) is limited to the attic,
and debris in the pocket can be cleaned.
(b) Stage 2: The cholesteatoma is limited to the attic,
but debris in the pocket (light gray area) cannot be cleaned.
(c) Stage 3: The cholesteatoma extends beyond the attic to invade the mastoid antrum.
The ossicular chain is buried in the cholesteatoma and disarticulated.
(d) Stage 4: The cholesteatoma widely destroys the posterior wall of the external auditory canal and invades the mastoid antrum,
mastoid air cells,
and tympanic cavity.

Fig. 8: Axial (a) and coronal (b) CT images of attic cholesteatoma (Stage 4) show soft tissue, which erodes the scutum and ossicles, in the Prussak’s space.

Fig. 9: Axial sequential CT images of advanced attic cholesteatoma (Stage 4) show destruction of the semicircular canals and cochlea.
♣Tensa cholesteatoma
Tensa cholesteatomas comprise 20% or fewer of acquired cholesteatomas,
occurring in the tympanic sinus or uncommonly as tensa retraction cholesteatoma.
In sinus-type cases,
CT shows soft tissue located medially to the ossicles and external displacement of the ossicles.
Postoperative recurrence is more frequent and postoperative hearing disturbance more severe in this type than the attic type.

Fig. 10: Axial (a) and coronal (b) CT images of tensa cholesteatoma show soft tissue, which erodes the incus, located medially to the ossicles.
♦Checkpoints
- soft tissue that erodes the ossicles (no ossicular erosion ⇒ most likely middle ear effusion,
not cholesteatoma)
- erosion of the scutum,
ossicles,
ossicular chain,
tympanic tegmen,
facial nerve canal,
semicircular canals/labyrinthine fistula and cochlea
♣External auditory canal cholesteatoma
External auditory canal cholesteatoma occurs when squamous tissue invades a localized area of periosteitis in the canal wall; its etiology and pathophysiology are unknown.
CT shows focal or diffuse soft tissue that erodes the wall of the external auditory canal,
especially the inferior or posterior wall.
The tympanic membrane is usually normal.
When cholesteatoma is limited to the external auditory canal,
local treatment is possible.
However,
invasion of cholesteatoma into the middle ear/mastoid requires tympanoplasty/mastoidectomy.

Fig. 11: (a) Axial CT image of the external auditory canal cholesteatoma shows soft tissue that erodes the external auditory canal, (b) opposite side (normal).
♦Checkpoints
- soft tissue that erodes the external auditory canal wall
- invasion to the middle ear,
mastoid cavity
♣Otosclerosis
The etiology of otosclerosis is unknown.
Otosclerosis is classified into fenestral and cochlear (or retrofenestral) types.
Patients present with progressive conductive (fenestral type) or mixed (fenestral and cochlear type) hearing loss with normal findings on otoscopic examination.
Fenestral otosclerosis spreads from the oval window anterior margin (fissula ante fenestram) to the all margin of oval and round windows.
Continued active disease spreads to the otic capsule (both fenestral and cochlear present).
Fixation of the stapedial footplate causes conductive hearing loss.
Fenestral otosclerosis usually occurs in young adults and is mostly (85%) bilateral.
In its early stage,
the most common CT finding is a lucent area just anterior to the stapedial footplate.
Later,
calcified foci may narrow or even obliterate the oval window.
Treatment consists of stapedectomy and insertion of a stapes prosthesis.
Cochlear (or retrofenestral) otosclerosis is much less common but always associated with fenestral otosclerosis.
Patients present with mixed conductive and sensorineural hearing loss.
Histologically,
foci of spongy new bone extend around the cochlea and sometimes even around the vestibule,
semicircular canals,
and internal auditory canal.
Cochlear otosclerosis is treated with sodium fluoride or a cochlear implant.
In cochlear otosclerosis,
CT shows focal lucencies in the otic capsule that may extend ring-like around the cochlea.
Later,
in the sclerotic phase,
these foci may undergo remineralization and become indistinguishable from the normal otic capsule.

Fig. 12: Combined fenestral and cochlear otosclerosis (bilateral)
CT shows bilateral “halo” of radiolucency surrounding the cochlea (arrows); also note the bilateral lytic lesions anterior to the oval window (broken arrows).
♦Checkpoints
- fenestral type: lytic lesions anterior to the oval window
- cochlea type: lytic lesions around the cochlea
♣Tympanosclerosis
Tympanosclerosis is thought to be a complication of otitis media in which deposits of hyaline cells,
calcium,
and phosphate crystals accumulate diffusely within the tympanic membrane and submucosa of the middle ear.
The disease is characterized by calcific,
bony,
or fibrous middle ear foci secondary to suppurative COM.
Tympanosclerotic plaques appear as a semicircular crescent or horseshoe-shaped white plaque within the tympanic membrane.

Fig. 13: Axial (a) and coronal (b) CT images of tympanosclerosis show destructive ossicles and calcification in the attic.
♦Checkpoint
- calcification of tympanic membrane,
ossicle surface,
stapes footplate,
muscle tendons,
or ossicle ligament
♣Trauma
Incudomalleolar joint separation is most frequently observed in trauma cases and often associated with incudostapedial joint separation [1].

Fig. 14: Axial (a) and coronal (b) CT images show hematoma in the tympanic cavity and malleoincudal disarticulations.
♦Checkpoints
- temporal bone fractures
- disarticulation of the ossicular chain
- injury of facial nerve canal
- perilymph fistula
♣Ossicular anomalies
Developmental disorders that involve the ossicles and originate in the first and second branchial arches cause various ossicular anomalies.
Stapes footplate fixation,
the most common,
cannot be diagnosed by CT [2,
3].
However,
absence of the upper part of the stapes or the long process of the incus can be diagnosed by CT.
Bilateral conductive deafness is an indication for surgical reconstruction (tympanoplasty).

Fig. 15: (a) Axial CT image shows absence of the posterior limb of the right stapes; (b) on the CT image of the opposite side (normal), the posterior limb of the right stapes (arrow) cannot be identified.

Fig. 16: Axial sequential CT images show incudostapedial disarticulation.
♦Checkpoints
- absence of some part of ossicles
- disarticulation of the ossicular chain
♣Fibrous dysplasia
Fibrous dysplasia is a bone disorder in which dysplastic fibro-osseus tissue replaces normal bone.
Radiologic findings are of 3 types−pagetoid (50%),
sclerotic (25%),
and cyst-like (25%).
In particular,
expansile “ground-glass” density is typical with bone CT.
Stenosis of the external auditory canal causes infection that leads to cholesteatoma and hearing loss.

Fig. 17: Axial CT image of fibrous dysplasia (pagetoid type) shows stenosis of the external auditory canal by expansile “ground-glass” density that invades the sphenoid and petrous bones.
♦Checkpoints
- pagetoid,
sclerotic,
and cyst-like changes of the temporal bone
- complicated by cholesteatoma
- stenosis of the external auditory canal
Sensorineural hearing loss
Imaging of sudden sensorineural hearing loss has traditionally been performed to rule out cerebellopontine angle masses,
but increasing technological sophistication of MRI has allowed the detection of inner ear abnormalities.
MRI should be performed in all cases of sudden sensorineural hearing loss with uncertain cause [4].
However,
some cases can only be diagnosed on T1-weighted images with contrast medium (small schwannoma,
suppurative otitis interna,
sudden deafness,
anterior inferior cerebellar artery infarct,
Ménière’s disease,
and others) or show no abnormality in CT/MRI images (some sudden deafness,
Ménière’s disease,
and others).

Fig. 18: Sample flow chart for diagnosing sensorineural hearing loss
Tumor
♣Vestibular schwannoma
Vestibular schwannoma is a benign tumor that arises when Schwann cells wrap the vestibular branches of CN8 in the cerebellopontine angle–internal auditory canal.
CT may miss smaller intracanalicular lesions (< 6 mm).
If multiple or bilateral schwanomas are seen,
neurofibromatosis type2 must be considered.

Fig. 19: MRI T2-weighted image (a) and T1WI with contrast medium (b) of acoustic nerve schwannoma show well enhanced small nodular lesion in the left internal auditory canal.
♦Checkpoints
- involve cochlear nerve canal
- multiple or bilateral schwannoma (neurofibromatosis type2 must be considered)
♣Facial nerve schwannoma
In the case of facial nerve schwannoma,
conductive or mixed hearing loss and sensorineural hearing loss both occur.
Conductive or mixed hearing loss easily occurs when a tumor progresses into a temporal bone (inside the tympanic cavity) from the geniculate ganglion of the facial nerve.
Symptoms are mild compared with sensorineural hearing loss,
and hearing is expected to improve with tumor resection.
On the other hand,
sensorineural hearing loss occurs when a tumor progresses to the internal auditory canal and cerebellopontine angle from the geniculate ganglion of the facial nerve.
Improvement of hearing loss is difficult because of damage to the inner ear or cochlear nerve.

Fig. 20: Axial sequential (a-d) and coronal (e) CT images of a facial nerve schwannoma. Bone CT shows expansile mass lesion in right mastoid air cells extruding to the external auditory canal and an enlarged stylomastoid foramen.
♦Checkpoint
- enlarged stylomastoid foramen/facial nerve canal (facial nerve schwannoma), internal auditory canal
♣Labyrinthitis ossificans (LO)
Labyrinthitis ossificans (LO) is the pathologic formation of new bone within the lumen of the otic capsule and associated with profound deafness and loss of vestibular function.
LO is the final result of suppurative labyrinthitis regardless of the origin of the infection [5].
Uncommon causes for LO include tumors,
advanced otosclerosis,
fracture of the temporal bone,
and hemorrhage of the inner ear [6].
LO causes profound hearing loss,
and the ossification process can prevent cochlear implantation (CI) [7,
8].
CT shows fibro-osseous changes or bony encroachment in the fluid space of the membranous labyrinth (cochlear/noncochlear).
Radiologists should describe LO as “cochlear” or “noncochlear” type,
because cochlear LO makes cochlear implantation problematic.
CT has greatly aided diagnosis of LO [9] and evaluation of the possibility of CI [10].

Fig. 21: Axial CT of labyrinthitis ossificans (b, d) and normal opposed side (a, c) show severe ossification of the cochlea, lateral semicircular canal, and vestibule.
♦Checkpoint
- fibro-osseous changes or bony encroachment in fluid space of membranous labyrinth “cochlear” or “noncochlear” type
♣Anomalies
Approximately 20% of patients with congenital sensorineural hearing loss have radiographic abnormalities of the inner ear [11].
Sennarogu and Saatcu [12] have proposed a classification system for inner ear malformations based on radiological features.
Classification of inner ear malformations
A) Cochlear malformation
- complete absence of all cochlear and vestibular structures (Michel deformity)
- cochlear aplasia
- common cavity malformation: cystic cavity representing the cochlea and vestibule; cochlea and vestibule cannot be distinguished.
- cochlear hypoplasia: further differentiation of the malformation allows differentiation of smaller than normal cochlea and vestibule; hypoplastic cochlea resembles a small bud off the internal auditory canal
- incomplete separation type 1: cystic appearance of the cochlea from absence of the entire modiolus and cribriform area accompanied by a large cystic vestibule
- incomplete separation type 2 (Mondini deformity): The cochlea consists of 1.5 turns,
in which the middle and apical turns coalesce to form a cystic apex,
accompanied by a dilated vestibule and enlarged vestibular aqueduct.
B) Normal cochlea
- vestibular malformations include Michel deformity,
common cavity, absent/hypoplastic/dilated vestibule
- semicircular canal malformations
- internal auditory canal malformations
- vestibular and cochlear aqueduct findings

Fig. 22: Axial sequential CT images show large vestibular aqueduct (allow), hyperplasia of the cochlea (arrowheads), and large lateral semicircular canal (broken allows); superior semicircular canal is normal.

Fig. 23: Axial MRI T2WI images show right enlarged lateral semicircular canal; superior/posterior semicircular canal is normal.

Fig. 24: MRI of T2WI (a–d) and volume-rendered images (e, f) show bilateral small common cavity (arrows) with narrow internal auditory canal (broken arrows) and hypoplastic semicircular canals (arrowheads).
♦Checkpoints
- cochlea aplasia/hypoplasia
- absent septation between middle and apical turns of the cochlea (< 2.5 turns)
- normal or mildly dilated vestibule
- large vestibular aqueduct ≥ 1 mm at midpoint
- large lateral semicircular canal ≥ 0.8 mm at midpoint




 and coronal (b) CT images of attic cholesteatoma (Stage 4) show soft tissue, which erodes the scutum and ossicles, in the Prussak’s space.")
 show destruction of the semicircular canals and cochlea.")
 and coronal (b) CT images of tensa cholesteatoma show soft tissue, which erodes the incus, located medially to the ossicles.")
 Axial CT image of the external auditory canal cholesteatoma shows soft tissue that erodes the external auditory canal, (b) opposite side (normal).")

CT shows bilateral “halo” of radiolucency surrounding the cochlea (arrows); also note the bilateral lytic lesions anterior to the oval window (broken arrows).")
 and coronal (b) CT images of tympanosclerosis show destructive ossicles and calcification in the attic.")
 and coronal (b) CT images show hematoma in the tympanic cavity and malleoincudal disarticulations.")
 Axial CT image shows absence of the posterior limb of the right stapes; (b) on the CT image of the opposite side (normal), the posterior limb of the right stapes (arrow) cannot be identified.")

 shows stenosis of the external auditory canal by expansile “ground-glass” density that invades the sphenoid and petrous bones.")

 and T1WI with contrast medium (b) of acoustic nerve schwannoma show well enhanced small nodular lesion in the left internal auditory canal.")
 and coronal (e) CT images of a facial nerve schwannoma. Bone CT shows expansile mass lesion in right mastoid air cells extruding to the external auditory canal and an enlarged stylomastoid foramen.")
 and normal opposed side (a, c) show severe ossification of the cochlea, lateral semicircular canal, and vestibule.")
, hyperplasia of the cochlea (arrowheads), and large lateral semicircular canal (broken allows); superior semicircular canal is normal.")

 and volume-rendered images (e, f) show bilateral small common cavity (arrows) with narrow internal auditory canal (broken arrows) and hypoplastic semicircular canals (arrowheads).")