1.
INFECTIOUS DISEASE
Urinary tract infections are the most common urologic diseases.
In the United States of America,
involving seven million doctor visits and one million visits to emergency departments.
It is the main differential diagnosis on ureteral colic.
1.1.
Acute pyelonephritis (APN)
In adult patients,
the diagnosis was based on clinical and laboratory data. Generally,
it is not necessary to perform any imaging in the early diagnosis of acute pyelonephritis.
Imaging tests are reserved for patients:
1.Unresponsive to treatment within 72 hours.
2.Patients as diabetics,
the elderly or immunocompromised.
3.To characterize the severity of the infection.
The first technique that we use is ultrasound, showing abnormalities in 24% of patients (fig.
2 and 3).
The main findings are:
1.
Increased kidney size
2.
Altered cortical echogenicity: this change in cortical echogenicity is due to both edema (hypoechoic) as bleeding (hyperchoic)
3.
Corticomedullary differentiation loss
4.
Compression of the renal sinus
5.
Presence of focal mass or abscess
6.
Areas of hypoperfusion in Doppler ultrasound

Fig. 2: A 50 years old woman presented the emergency department by epigastric abdominal pain radiating to the right upper quadrant, nausea and bilious vomiting, 20.76 leukocytes (neutrophils 89.1%). Pyuria, pyuria and bacteriuria
In US, there are focal hyperchoic cortical, corticomedullary differentiation loss and compression of the renal sinus (arrows).
The diagnosis was acute pyelonephritis in the right kidney with multisensible E.coli in hemocultures.
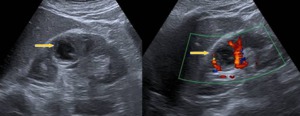
Fig. 3: A 67 years old woman with bilateral nephrolithiasis. Ten-day history of asthenia, decreased appetite and colic left lumbar pain with voiding symptoms flowery. In the last two days, she has fever with shivering too. In ultrasound demonstrated the presence of a right renal abscess, with multisensible E. coli in urine and blood culture. After 12 days of treatment, there gradually decrease the size of the abscess.
The Computed Tomography (CT) scan with intravenous contrast is the study of choice. The postcontrast study is acquired between 50-90 seconds and the late study is performed if there is suspicion of obstruction of the excretory system.
The main findings that we can find at the CT are:
1.
Increased kidney size
2.
Cortical areas of low attenuation,
well defined triangular morphology (fig.
4)
3.
Perirenal bands and thickened Gerota's fascia (fig.
5)
4. Striated enhancement
5.
Renal abscess: in 75% of cases are diabetic patients (fig.
6)
6.
Perinephric abscess,
usually in the psoas
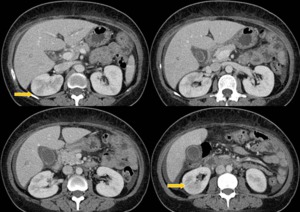
Fig. 4: A 50 years old woman with the diagnosis was acute pyelonephritis in the right kidney with multisensible E.coli in hemocultures.
She does not good performance with antibiotic treatment. CT is requested with cortical areas of low attenuation (arrows).
The patient had inflammation of gallbladder wall and free fluid without signs of cholecystitis.
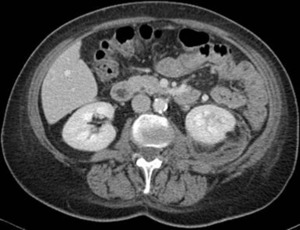
Fig. 5: Acute pyelonephritis in left kidney with perirenal fluid and thickened Gerota's fascia

Fig. 6: A 67 years old woman with bilateral nephrolithiasis. Ten-day history of asthenia, decreased appetite and colic left lumbar pain with voiding symptoms flowery. In the last two days, she has fever with shivering too. In CT demonstrated the presence of a right renal abscess (arrow).
1.2.
Emphysematous pyelonephritis
This is a severe necrotizing infection with gas formation within and surrounding the kidney.
In 90% of cases,
are poorly controlled diabetic patients,
but is also associated with urinary tract obstruction and immunocompromised patients. It is a disease more common in women over age 60 years old.
The most common bacteria are E.
coli,
Klebsiella pneumoniae and Proteus mirabilis.
We can summarize the findings in different imaging techniques:
1.
X-ray of abdomen can find gas in flank.
2.
Ultrasoundcan see renal increase and echogenic foci of gas with dirty shadow.
3.
CT is the study of choice: It identifies the rise and destruction of the kidney,
speckled or linear gas,
fluid levels and focal necrosis.
Emphysematous pyelitis is the least aggressive of emphysematous infection of the upper urinary tract.
It is defined by the presence of gas located in the renal collecting system.
Imaging techniques (abdominal radiography,
ultrasound and CT) show the presence of gas bubbles or air-fluid levels in calyces,
ureter and renal sinus (fig.
7).

Fig. 7: A 83 years old male with polycystic kidney and ureteropelvic junction stenosis known. Right flank pain, dysuria, and leukocytosis. Abdominal CT was performed with suspected urinary sepsis.
The diagnosis is emphysematous pyelitis, with gas in calyces and renal pelvis (arrows). Treatment of the patient's bladder catheterization and antibiotic (Piperacillin-Tazobaztam), with resolution of the symptoms. In urine culture grew > 100,000 CFU / ml of Enterococcus faecalis and Escherichia coli.
1.3.
Emphysematous cystitis
This condition occurs in older women with diabetes.
The most common symptom is abdominal pain.
Medical treatment is with antibiotics,
probing and debridement bladder washings.
It is rarely necessary total or partial cystectomy.
The mortality rate is 7% (fig.
8).

Fig. 8: A women 94 years old with sweating, shivering, drowsiness and periumbilical pain. In recent days she has smelly urine. Leukocytosis of 33,000. Abdominal CT is performed for urinary sepsis. Gas is identified in the bladder wall with no history of bladder instrumentation with emphysematous cystitis. Continued sustained fever, despite antibiotic therapy with progressive decrease in the level of consciousness and dies.
1.4.
Pyonephrosis
It is the infection of dilated urinary excretory system.
The causes of this dilatation can be varied: stones,
tumors,
benign stricture or papillary necrosis.
The pyonephrosis should be suspected in patients with known obstruction,
fever and flank pain.
The findings in the different imaging techniques are:
1.
X-ray of abdomen may appear in location renal mass.
2.
Ultrasound is displayed dilation of the excretory system,
the presence of fluid-fluid levels,
and the presence of echogenic debris (fig.
9).

Fig. 9: Ultrasound of women with known strictures binding pielouretal with fever and left flank pain. Presents dilated calyces with thick walls and a few with echoes inside corresponding with severe pyonephrosis
3.
In abdominal CT,
we can visualize the collecting system dilatation,
wall thickening of pelvis and ureter,
with renal and perirenal inflammatory changes (fig.
10).

Fig. 10: In abdominal CT, we see the wall thickening of pelvis and ureter (orange arrows), with renal and perirenal inflammatory changes (blue arrow) in left pyonephrosis.
2.
Renoureteral colic.
The first cause of this clinical pathology is urinary tract obstruction by the presence of a stone.
The effort and skill of the radiologist should aim to demonstrate the stones,
determine the size and location and identify complications.
Abdominal plain radiography is the first imaging technique to be performed.
Recent studies show a 48-62% sensitivity in the detection of calculation if the X-ray is performed by radiologists (fig. 11).
If abdominal radiography determine the size and location,
are not precise another imaging techniques.

Fig. 11: Abdominal X-ray with left ureteral stone (arrow)
The indication for other imaging techniques is:
1.
Persistent pain.
2.
The onset of fever and worsening renal function
3. No visualization of the stone.
Ultrasound is the next imaging technique that we can use.
It allows the assessment of the renal parenchyma,
the presence of hydronephrosis and detecting stones with a specificity of 93-95% and a sensitivity of 19-97% (fig.
12).

Fig. 12: A 34 years old male presented the emergency department with left lumbar pain with previous renal colic. Pain is resistant to analgesic treatment and presents creatinine elevation respect previous analytical.
In ultrasound, we identified excretory system dilatation (orange arrow)and a stone in left meatus (blue arrow).
If the ultrasound shows no stones,
computed tomography (CT) without intravenous iodinated contrast is the diagnostic test of choice.
It allows detection of urolithiasis and determines the indirect signs of the impact on the urinary tract.
We recommend low-dose studies,
although the CT can underdiagnose smaller stones that 3 mm, lithiasis in the vesicoureteral junction and in obese patients.
In patients older than 60 years with normal unenhanced CT,
we recommend the use of intravenous contrast to rule out vascular pathology.
The direct sign that we value in the CT without iodinated contrast is the detection of urolithiasis,
with sensitivity and specificity above 95% (fig.
13).

Fig. 13: Unenhanced abdominal CT with a small stone in the middle third of the left ureter.
The size and location of the stone are the determining factors in the clinical management,
ranging from simple analgesia,
medical expulsive therapy or endoscopy.
Indirect signs that we analyze in abdominal CT are (fig.
14):
1.Hydronephrosis and hydroureter.
2.Perirenal bands: lines of increased density in the perirenal fat.
3.The ring sign: presence of visible ureteral wall surrounding the stone as local inflammatory response (fig.
15).

Fig. 14: Unenhanced abdominal CT with hydronephrosis and hydroureter (double green arrow)and perirenal bands (blue arrow)

Fig. 15: Unenhanced abdominal CT with the ring sign, identifying thickening of ureter wall surrounding the stone.
The contrast-enhanced CT should be performed if:
1.
Unilateral perirenal crosslinking without hydronephrosis.
2.
Complicated mass or cyst.
3.
In patients with hematuria and normal unenhanced CT.
4.
Presence of perirenal collection.
3.
VASCULAR PATHOLOGY
3.1.
Wunderlich syndrome
It is defined as spontaneous nontraumatic renal bleeding confined to subcapsular and perirenal space.
The causes of this condition are numerous.
The most frequent causes are a tumor (57-66%),
especially angiomyolipomas,
renal cell carcinoma and urothelial carcinoma.
Vascular diseases are 18% (polyarteritis nodosa, drugs vasculitis) and inflammatory processes.
Patients may present the classic triad of Lenk with lumboabdominal acute pain,
palpable mass and hypovolemic shock.
The imaging techniques that we can used are:
1.
Ultrasound can identify a heterogeneous mass,
allowing the suspected diagnosis,
but not the etiology.
2.
Abdominal CT: The best technique to establish the diagnosis and etiology.
It identifies a mass with hyperdense areas (> 60 HU) precontrast study,
allows assessing the existence of active bleeding in CT with intravenous iodinated constrast. If we can detect fat density intrahematoma,
we suspect angiomyolipoma as source of bleeding (fig.
16).
3.
Arteriography allows embolization of the bleeding vessel.
3.2.
Thrombosis of renal vessels
The renal artery thrombosis is secondary to emboli from the left heart (fig.
17),
aortic dissection,
trauma,
renal aneurysm,
arteriosclerotic stenosis of renal artery or iatrogenic origin.
Acute renal ischemia produces renal infarction more or less extensive,
according to the existence of collateral circulation (fig.
18).

Fig. 17: A 36 years old male with mitral prosthesis presents fever, abdominal pain and hypotension. He presents endocarditis in echocardiography. Abdominal CT with intravenous contrast showing splenomegaly and splenic hypodense infarct areas (blue arrows). Also displayed bilateral renal infarctions (orange arrows) and contrast extravasation in the right psoas muscle consistent with active bleeding (red arrows)

Fig. 18: A 65 years old male with ischemic heart disease, arterial ischemia of lower limbs and organized mural thrombus in cardiac apex. He presents left flank pain. The abdominal CT shows thrombosis of the left renal artery and infarction (arrow)
The renal vein thrombosis may be secondary to thrombophlebitis extending from the inferior vena cava, the renal vein invasion by renal neoplasms,
trauma,
post-surgical injuries,
pregnancy or use of oral contraceptives.
4.
INJURIES
4.1.
Renal trauma
Urinary injuries account for 3-10% of abdominal trauma.
The lesions are associated in 80-90% to blunt abdominal trauma,
often associated with other organ damage.
The 95% of patients present hematuria,
flank pain,
anuria or ecchymosis.
We must remember that the degree of hematuria does not correlate with the severity of renal injury.
The technique of choice is abdominal CT with intravenous contrast,
especially in blunt abdominal trauma with:
1.
Hematuria.
2.
Microscopic hematuria and hypotension.
3.
Blunt trauma in patients with rapid deceleration,
fall from height,
flank hematoma,
lower rib or thoracolumbar spine fractures.
The abdominal CT protocol may include a non-contrast study if there is suspicion of active bleeding or renal hematoma.
It is essential an arterial and nephrographic phase.
The elimination phase with delayed 5 minutes and low dose radiation can assess vascular pedicle injuries,
evaluating the excretory system or the distinction between active bleeding and pseudoaneurysm.
It uses the classification of renal damage of American Association for the Surgery of Trauma (AAST),
based on the appearance of kidney surgery.
AAST Grade I: These are the most common injuries (75-85%) and include:
1.
Hematuria with normal CT.
2.
Contusion: ovoid or rounded areas are ill-defined with low density (fig.
19).
3.
Subcapsular hematoma: It is no associated with renal laceration and it is less frequent than perirenal hematomas.

Fig. 19: Abdominal CT with intravenous iodine contrast showing ovoid hypodense area in the anterior cortex of the left kidney corresponding to contusion (arrow).
AAST Grade II: Includes
1.
Perirenal hematoma: collection confined between the renal parenchyma and Gerota's fascia.
It is associated with thickening of the fascia lateroconal,
colon compression and displacement of the kidney (fig.
20).

Fig. 20: Abdominal CT showing a hypodense collection between the left kidney and Gerota's fascia corresponding to perirenal hematoma (arrow).
2.
Cortical laceration: hypodense linear defects are less than 1 cm, without excretory system damage (fig.
21).

Fig. 21: Abdominal CT showing a linear hypodense image in the anterior cortex of the left kidney related to renal laceration less than a centimeter (arrow).
AAST Grade III: The cortical lacerations are larger than 1 cm without excretory system damage (fig.
22).

Fig. 22: Abdominal CT showing a linear hypodense image in the posterior cortex of the left kidney related to renal laceration more than a centimeter(arrow). It corresponds to a grade III injury of AAST classification and it is associated with perirenal hematoma.
AAST Grade IV: Includes several injuries
1.
Lacerations with involvement to the collecting system and urine extravasation perirenal space
2.
Segmental infarct due to thrombosis,
dissection or laceration of a intrarenal or capsular branch.
They are well-defined areas with base in the renal capsule and the apex in the renal hilum (fig 23).

Fig. 23: Abdominal CT with coronal and axial images that show a large right renal infarction in patient with abdominal trauma and flank pain.
AAST Grade V:
1. Renal fracture is identified with multiple fragments,
devitalized areas,
excretory system injuries, and blood active bleeding (fig.
24).
2.
Renal vascular pedicle avulsion.

Fig. 24: Abdominal CT with intravenous contrast that shows a renal fracture (arrows) with perirenal hematoma
4.
2.
Bladder trauma
The 10% of pelvic fractures are associated with bladder rupture. Only a third of bladder ruptures are located adjacent to the pelvic fracture.
5.
COMPLICATIONS
The frequency and extent of complications are related to the degree of complexity of surgical and laparoscopic procedures,
accepting overall complication rate of 7%.
Bleeding complications were most frequent at nephrectomy and laparoscopic radical prostatectomy.
We found hematomas in the bladder wall after suprapubic puncture (fig.25).

Fig. 25: A male 70 years with radical prostatectomy for neoplasia. He presents urethral stenosis, unable to perform optical urethrotomy. Bladder puncture is performed and the patient complained of suprapubic pain within hours. Abdominal CT shows a paravesical lesion in relation with hematoma on the right wall of the bladder(arrow).
Major vascular injuries were also presented during complex surgeries adrenalectomy,
nephrectomy and retroperitoneal lymphadenectomy.
Also occur suture dehiscence and postoperative abscesses after laparoscopic prostatectomy (fig 26 y 27).

Fig. 26: A 66 years old male with radical laparoscopic prostatectomy. He has abdominal pain resistant to analgesia. There are output of urine by the drainages. Abdominal CT shows intravesical contrast extravasation (arrows) by dehiscence bladder neck, confirmed at surgery.

Fig. 27: A 62 years old man with radical prostatectomy for carcinoma. He has a fever and pelvic pain. Abdominal CT shows a large abscess in pelvis (green arrow), which required percutaneous drainage, with good outcome.
Oncological patients often consulted in the emergency department for urological reasons.
The cause of hematuria more characteristic of the oncology patient is hemorrhagic cystitis after chemotherapy (fig.
28) or radiotherapy.
It is more rare secondary hemostasis disorders,
thrombocytopenia or viral cystitis.

Fig. 28: A 51 years old male with myelodysplastic syndrome undergoing bone marrow transplantation. He is being treated with cyclophosphamide and begins with dysuria and hematuria. The abdominal CT shows thickening of the bladder walls, contained hyperdense material in relation to hemorrhagic cystitis, which was confirmed by cystoscopy.
Cyclophosphamide (specifically urinary metabolite,
acrolein) produces hematuria up in 65-70% of patients.
Is usually mild and can be managed with conservative measures,
but can be massive.
6.
PEDIATRIC UROLOGICAL EMERGENCY
Pediatric patients have different urological conditions that may require imaging techniques.
The main indications are:
- Abdominal pain with symptoms nephrourologic
- Low infection
- Pyelonephritis
- Bacteriuria / Hematuria
- Oliguria / polyuria
- Complications of renal transplantation
- Injuries
The technique of choice is the ultrasonography (fig.
29),
with significant support from Doppler study.
In selected cases and renal trauma,
it may be necessary to perform abdominal CT.

Fig. 29: A girl 4 months old. In prenatal ultrasound, she has a double collecting system and right hydronephrosis. She comes to the emergency department with fever and lethargy.
Ultrasound shows dilated double excretory system with echogenic content related to right pyonephrosis.
References: Courtesy of Dr. G. Albi. Hospital Universitario Niño Jesús (Madrid, Spain)
7.
UROLOGICAL EMERGENCIES IN THE PREGNANT PATIENT
Pregnant patients can have any of the conditions reported previously.
Moreover,
we must know a specific pathology: the symptomatic hydronephrosis of pregnancy.
Hydronephrosis have variable incidence: appears in the first trimester by 15% and increases to 50% in the third trimester.
It affects the right than the left kidney (fig.
30). The technique of choice for the diagnosis and monitoring is the ultrasonography.
In selected cases,
it may be necessary to perform MRI with sequences T2.

Fig. 30: A female 31 years old with 26 weeks gestation. She has abrupt colicky pain in the right flank, which is resistant to analgesia. She has hematuria with 3-4 erythrocytes per field.
In ultrasound identifies pelvicalyceal dilatation and the right ureter without lithiasis. We performed a renal ultrasound control at eight weeks after birth, showing normal kidneys without evidence of pelvicalyceal dilatation.

. Pyuria, pyuria and bacteriuria
In US, there are focal hyperchoic cortical, corticomedullary differentiation loss and compression of the renal sinus (arrows).
The diagnosis was acute pyelonephritis in the right kidney with multisensible E.coli in hemocultures.")

.
The patient had inflammation of gallbladder wall and free fluid without signs of cholecystitis.")

.")
. Treatment of the patient's bladder catheterization and antibiotic (Piperacillin-Tazobaztam), with resolution of the symptoms. In urine culture grew > 100,000 CFU / ml of Enterococcus faecalis and Escherichia coli.")


, with renal and perirenal inflammatory changes (blue arrow) in left pyonephrosis.")
")
and a stone in left meatus (blue arrow).")

and perirenal bands (blue arrow)")


. Also displayed bilateral renal infarctions (orange arrows) and contrast extravasation in the right psoas muscle consistent with active bleeding (red arrows)")
")
.")
.")
.")
. It corresponds to a grade III injury of AAST classification and it is associated with perirenal hematoma.")

 with perirenal hematoma")
.")
, which required percutaneous drainage, with good outcome.")

")

 by dehiscence bladder neck, confirmed at surgery.")