ECR 2013 / C-1128
Abdominal Hydatidosis – Imaging Features
Congress:
ECR 2013
Poster Number:
C-1128
Type:
Educational Exhibit
Keywords:
Abdomen, Liver, Kidney, Ultrasound, CT, MR, Diagnostic procedure, Education, Comparative studies, Parasites, Infection, Cysts
Authors:
N. Neto, T. Saldanha; Lisbon/PT
DOI:
10.1594/ecr2013/C-1128

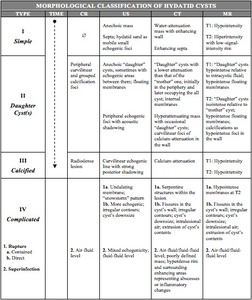
Table 1:
Classification of hydatid cysts on the basis of their appearance. Adapted from...

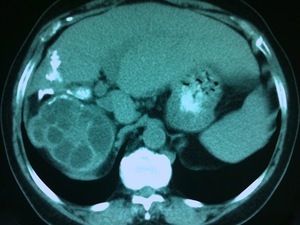
Fig. 1:
An 83-year-old woman presented two type I HC in the liver at US scan, the...

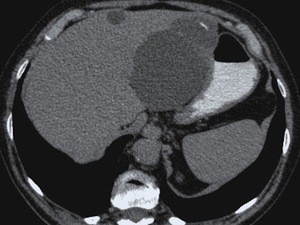
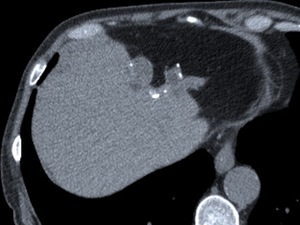
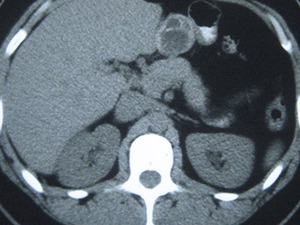
Fig. 2:
The same lesion as in figure 1 at contrast-enhanced CT, was low-attenuated with...

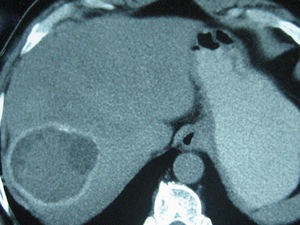
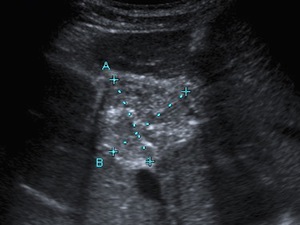
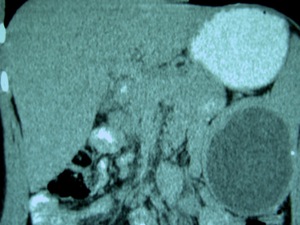
Fig. 3:
A type II hepatic HC incidentally found in a 71-year-old asymptomatic man at an...

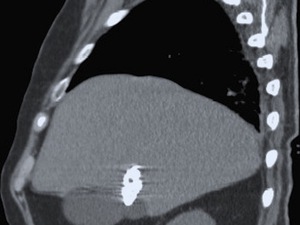
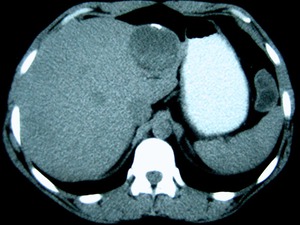
Fig. 4:
A large type II HC at an unenhanced CT scan, of higher attenuation than that of...

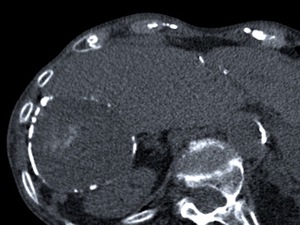
Fig. 5:
The same lesion as in figure 4 at CR, showed almost complete calcification of...

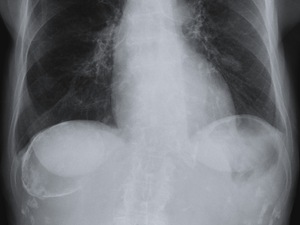
Fig. 6:
Round calcified mass in the right hypochondrium detected at abdominal CR...

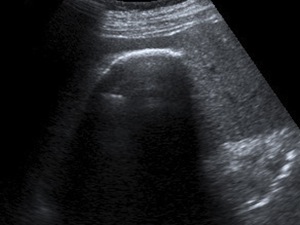
Fig. 7:
US scan of the same patient as in figure 6 showed a curvilinear echogenic line...

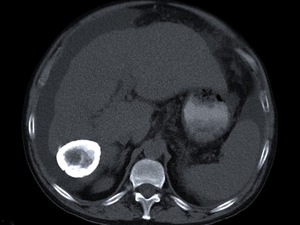
Fig. 8:
The same lesion as in figures 6 and 7 at an unenhanced CT scan appeared as an...
.")
Fig. 9:
Another old cyst, totally calcified, at an unenhanced CT scan of an...

Fig. 10:
Type II HC after a direct rupture, probably due to the left hepatectomy noted...

Fig. 11:
The same lesion as in figure 10, also evident at CR, due to the extensive...

Fig. 12:
Later after a direct rupture, HC become collapsed and calcified, as shown at...

Fig. 13:
The unenhanced CT scan of a patient with fever and abdominal pain with a known...

Fig. 14:
The abdominal US scan of a 41-year-old woman with hepatic and splenic disease...

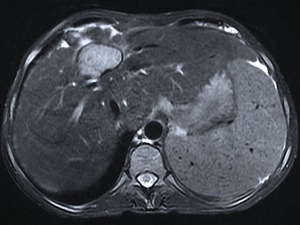
Fig. 15:
The same lesion as in figure 14, seen at this T2 weighted MR image was...

Fig. 16:
The same lesion as in figures 14 and 15 at T1 weighted images, presented...

Fig. 17:
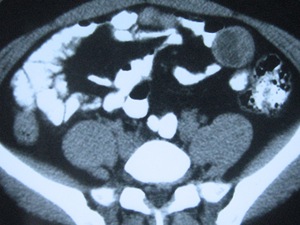
Hydatid peritoneal seeding in a 34-year-old woman, who underwent a CT scan for...

Fig. 18:
Mesenteric HC in the same patient as in figure 17.

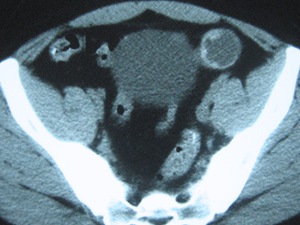
Fig. 19:
Type II HC in the left iliac fossa of the same patient as in figures 17 and

Fig. 20:
Type I HC with hyperdense hydatid sand in its dependent portion, detected in...

Fig. 21:
Intrasurgical photograph of mesenteric HC of the same patient as in figures 17...

Fig. 22:
Photograph of the surgical specimens of the same patient as in figures 17 to...

Fig. 23:
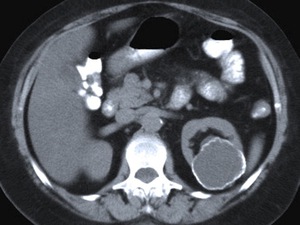
Renal HC in a 78 year-old woman with long-standing hepatic HD at an unenhanced...

Fig. 24:
Primary renal hydatidosis in a 46 year-old woman who presented with left flank...

Fig. 25:
Primary splenic HC in a 24-year-old woman, who underwent imaging examinations...

Fig. 26:
The same lesion as in figure 25 was also evident at the CT scan corresponding...

Fig. 27:
Coronal CT slice of the same lesion as in figures 25 and 26, showing the...