1.The body changes in pregnancy at MR imaging
Before interpreting images for pathologic findings in the pregnant patient,
it is necessary to understand the normal anatomy of the pregnant pelvis at multiplanar MR imaging and pregnancy associated anatomic changes.
The first trimesters
- The uterus maintains its normal version and flexion(fig.2-a).
- The bladder lies immediately anterior and inferior to the uterus.
- The vagina is posterior to the bladder and urethra and anterior to the rectum and anus.
- The ovaries lie within the pelvis lateral to the midline uterus and are suspended by the mesovarium,
broad ligaments,
and suspensory infundibulopelvic ligaments.
The second and third trimesters of pregnancy
- The gravid uterus increases in size and displaces the pelvic contents from their normal locations(fig.2-b).
- The adnexal structures are displaced superiorly and laterally.
- The appendix is often superiorly displaced from its normal position(fig.3).

Fig. 2: (a)Sagittal T2-weighted SSFSE image shows the uterus maintains its normal version and flexion.(b)Sagittal T2-weighted SSFSE image shows the gravid uterus increases in size and displaces the pelvic contents from their normal locations.
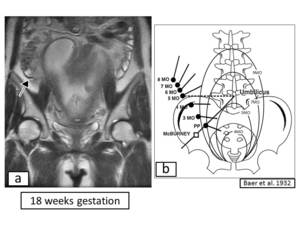
Fig. 3: (a)Coronal T2-weighted SSFSE images show superior displacement of the cecum and appendix by the gravid uterus. (b)The rise of the appendix and the fundus of uretus during pregnancy.
References: Baer et al.1932
2.Changes in pregnancy can confound the clinical diagnosis
Diagnosis of abdominal pain in pregnant women is confounded by several factors found in a normal pregnancy.
1.Uterus enlarges–Displacement of intraabdominal organs from their
normal locations.
2.The loss of elasticity in the abdominal wall musculature–Guarding in the
setting of peritonitis may not occur.
3.Nausea,
vomiting,
anorexia accompany normal pregnancy.
4.Physiologic alterations of laboratory values during pregnancy(fig.4)
–mild leukocytosis–physiologic anemia of pregnancy
–mild dilutional hypoalbuminemia
–mildly increased alkaline phosphatase level
–electrolyte changes
–particularly mild hyponatremia
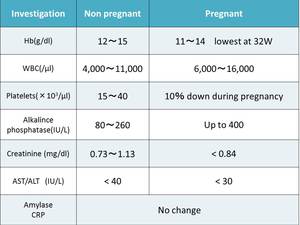
Fig. 4: Biochemical and haematological changes during pregnancy
References: 2.Mayer IE et al. Abdominal pain in pregnancy. Gastroenterol Clin North Am 1998; 27:1–36
3.Strategy of diagnostic imagings in pregnant patients
The clinical diagnosis of an intraabdominal disease in pregnant women is often obscured by concurrent maternal physiologic and anatomic changes.
Diagnostic imagings that takes into account the influence of the mother and fetus is required to decide treatment plan .
It is necessary to select the imaging procedure that takes into account the impact on the fetus due to exposure and use a contrast agent.
①Ultrasound during pregnancy
Ultrasound is widely used as the initial diagnostic imaging technique
during pregnancy because of its availability,
portability,
and lack of
ionizing radiation.
Unfortunately,
the test sensitivity depends on operator
technique,
patient cooperation,
and patient anatomy,
in that sensitivity
is decreased by abdominal fat and intestinal gas.
②CT imaging during Pregnancy
Diagnostic computed tomographic (CT) imaging is sometimes necessary
in a pregnant patient.
When a radiologist needs to decide if the diagnostic benefits will
outweigh the risks of radiation,
it is important to have a reasonably
accurate estimate of the radiation dose that the conceptus will receive.
The effects of radiation on the fetus are dependent on the gestational
age and radiation dose.
Organogenesis occurs predominantly between 2 and 15 weeks gestation.
Teratogenesis have a threshold of 100-200 mGy or higher and are
typically associated with central nervous system problems(fig.
).
Fetal doses of 100 mGy are not reached even with 3 pelvic CT scans or
20 conventional diagnostic x-ray examinations(fig.
).
The fetus is exposed to iodinated contrast media because the contrast
agent crosses the placenta.
Depression of fetal thyroid function is a potential harmful effect that can
be produced by exposure of the fetal thyroid to free iodide.
The intravascular use of non-ionic contrast media has been reported to
have no effect on neonatal thyroid function.
But,
in general,
intravascular contrast media should be avoided in
pregnancy,
in order to avoid any possible hazard to the fetus.
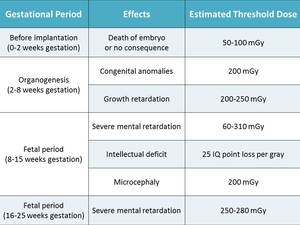
Fig. 5: Effects of Gestational Age and Radiational Dose on Radiation-induced Teratogenesis
References: ICRP Publication 84
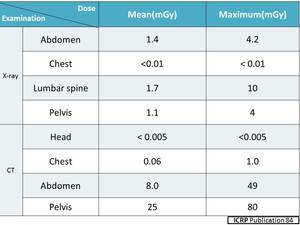
Fig. 6: Approximate fetal doses from fluoroscopy
References: ICRP publication
③MR Imaging during Pregnancy
MRI is also a useful technique for imaging pregnant patients given the
lack of ionizing radiation.
To date,
no deleterious effects to the developing fetus exposed to MRI
have been reported.
Therefore,
no specific consideration for MRI during the first,
second,
or
third trimester has been recommended.
The patient can be informed that there are no known harmful effects
from use of clinical MR imaging to date,
at 1.5T or lower magnetic field
strengths.
There is lack of experience with use of field strengths greater than 2.5T,
and they should be avoided at present.
Gadolinium-based MR contrast agents are known to pass through the
placenta to the fetal circulation.
To date,
no large,
well-controlled studies have been performed to
document the presence or absence of adverse fetal effects resulting from
maternal gadolinium administration.
The American College of Radiology (ACR) recommends iodineated
contrast administration during pregnancy only when it is deemed
necessary for prompt and accurate evaluation of the pregnant patient’s
medical condition.
The field of view for the examination extends from the dome of the
liver superiorly through the symphysis pubis inferiorly.
The protocol should include
a.
Axial,
sagittal,
and coronal T2-weighted SSFSE sequences
b.
Axial true fast imaging with steady-state precession (FISP)
sequences
c.
Axial in-phase and out-of-phase T1-weighted GRE sequences
d.
Axial short tau inversion-recovery (STIR) sequences
④Strategy of diagnostic imagings
Ⅰ. Ultrasound and MRI are not associated with known adverse fetal
effects.
Ⅱ. MRI has been no evidence of harmful effects at 1.5T or lower.
Ⅲ.
Exposure to < 50 mGy has not been associated with an increase
in fetal anomalies or pregnancy loss.
Ⅳ.
During pregnancy,
other imaging procedures not associated with
ionizing radiation should be considered instead of X-rays when
appropriate.
Ⅴ. Paramagnetic contrast agents are unlikely to cause harm and may
be of diagnostic benefit,
but these agents should be used during
pregnancy only if the potential benefit justifies the potential risk to
the fetus.
4. Acute abdomen in Pregnancy
Ectopic Pregnancy
Ectopic pregnancy,
which remains the most frequent obstetric cause of death in pregnancy,
often presents with abdominal or pelvic pain in the first trimester.
Heterotopic pregnancy is rare in the general population (1 in 7,000).
Risk factors for ectopic pregnancy,
advanced maternal age,
prior pelvic inflammatory disease (PID),
tubal surgery,
laboratory assisted reproduction,
previous abortion,
endometriosis,
preexisting fallopian,
adnexal,
or uterine pathology,
and prior complicated abdominal surgery,
such as ruptured appendicitis.
CT
CT scan findings are nonspecific for ectopic pregnancy.
The associated ionizing radiation poses a hazard if a normal
intrauterine pregnancy is present.
CT scanning is typically not an appropriate imaging modality to be
used for the analysis of ectopic pregnancy.
US
Ultrasound plays an instrumental role in ruling out an ectopic
pregnancy if it can confirm an intrauterine pregnancy.
Findings of an extrauterine ectopic pregnancy include the following:
1.
Live,
extrauterine embryo
2.
Absence of an intrauterine gestational sac
3.
Free fluid (particularly hemorrhagic) in the pelvis or peritoneum
4.
Adnexal mass
5.Hematosalpinx
6.Adnexal ring sign and a "ring-of-fire" sign on color Doppler
MRI
MRI can be used as a problem-solving technique for the less common
nontubal forms of ectopic pregnancies when sonography is
indeterminate.
In addition,
MRI can help differentiate between eccentric implantation
in the endometrium versus an interstitial ectopic pregnancy.
MRI is accurate in the characterization of tissue and in the detection
and age determination of blood products.
Findings that can suggest an ectopic pregnancy include the presence
of
1. A tubal gestational sac
2.
A tubal hematoma,
which is a hematoma suggested by the ring
sign (peripheral hyperintensity) on T1-weighted images
3. Tubal wall enhancement4.An adnexal mass with hemorrhagic fluid
in the peritoneum. Blood is suggested by the presence of high-
signal-intensity fluid on T1-weighted images.
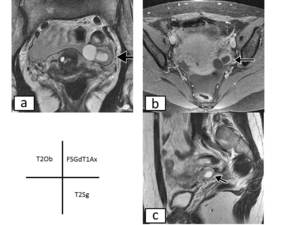
Fig. 7: Ectopic pregnancy at 6 weeks gestation.
(a)Oblique T2-weighted image,(b)Fat saturated Contrast-enhanced T1-weighted image,(c)Sagittal T2-weighted image shows eccentric intrauterine gestational sac that is not surrounded by endometrium.
Adnexal Masses
Adnexal masses occur in approximately 2% of all pregnancies.
Adnexal masses are not a usual cause of pain,
with 65% of these masses being asymptomatic and discovered incidentally on physical examination or sonography.
The size of the mass also does not necessarily dictate whether it will cause pain.
However,
if an adnexal mass is compressed,
if it compresses an adjacent organ or organs,
as is more likely to occur during pregnancy in association with an enlarging gravid uterus,
or if it becomes complicated by torsion,
hemorrhage,
or rupture,
the adnexal mass may present with pain.
Imaging evaluation of the adnexa should be performed,
starting with ultrasound,
in all pregnant women presenting with pain.
The most common adnexal masses during pregnancy are corpus luteum or other functional ovarian cysts.
The differential diagnosis for a complex-appearing adnexal mass includes hemorrhagic corpus luteum cyst,
ovarian cystadenoma,
and ovarian teratoma.
However,
approximately 1–8% of adnexal masses found during pregnancy are malignant .
US
Ultrasound provides the ability to distinguish adnexal masses that are small,
uncomplicated,
and likely to spontaneously resolve from those that appear larger and more complex with a higher likelihood of malignancy,
torsion,
or persistent pain from mass effect during pregnancy.
MRI
When the sonographic appearance of an adnexal mass is not specific,
MRI can be used for further characterization to help determine patient management during pregnancy.
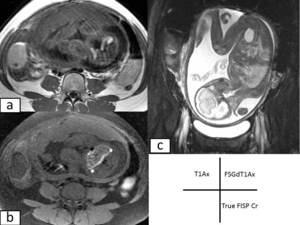
Fig. 8: Mature ovarian teratoma in a 29-year-old pregnant patient at 28 weeks gestation.a)Axial T1-weighted image,b)Axial Fat saturated contrast-enhanced T1-weighted image,c)Coronal true FISP image show a right ovarian mass that contains fat and fluid.
On the fat-saturated image, note the loss of the high signal
intensity in the macroscopic fat component of the mass.
Ovarian Torsion
The incidence of ovarian torsion is increased during pregnancy,
complicating 1 in 800 pregnancies.
Up to 7% of adnexal masses reportedly result in ovarian torsion during pregnancy.
Ovarian torsion most commonly occurs between 6 and 14 weeks’ gestation when uterine enlargement is most rapid.
However, up to 45% of cases of ovarian torsion presented during the second and third trimesters.
Ovarian torsion occurs more often in the right adnexa,
presumably because the sigmoid colon limits the mobility of the left ovary.
US
Ultrasound is the imaging modality of first choice.
But,
in the second and third trimesters of pregnancy,
the ovaries are
sometimes difficult to visualize US,
because they are displaced from
the pelvis by the enlarging uterus.
Findings that can suggest the ovarian torsion include the following
1. Enlarged hypo or hyperechoic ovary
2. Peripherally displaced follicles
3. Color doppler depicts an enlarged ovary without perfusion of the
parenchyma.
4. Free pelvic fluid
5. Whirlpool sign of twisted vascular pedicle
6. Underlying ovarian lesion can often be found
CT
1. Good at ruling out ovarian torsion if a normal ovary is seen
2. Torsion appears as a complex adnexal lesion representing:
–enlarged ovary
–distended pedicle
–possible underlying ovarian lesion
3. HU > 50 on non-contrast CT suggests haemorrhagic necrosis
4. Lack of enhancement
5. Surrounding fat stranding edema and free fluid
MRI
Usually not the imaging modality of choice as urgent imaging is
required.
-tube thickening
-Ovarian cystic mass
-Ascites
-Deviation of the uterus
-Hemorrhage and hemoperitoneum
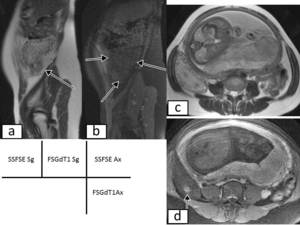
Fig. 9: Ovarian torsion in a 30-year-old pregnant patient.(a)Sagittal and (c)T2-weighted SSFSE image show an enlarged right ovary containing a mixed cystic-solid mass.
(b)Sagittal fat saturated contrast-enhanced T1-weighted image show the twisting of the vascular pedicle.
(d)Axial fat saturated contrast-enhanced T1-weighted image show haemorrhagic corpus luteal cysts.
Pathologic analysis
demonstrated ovarian torsion with ovarian edema,
with a serous cystadenofibroma as the lead point.
Leiomyomas
Uterine leiomyomas are commonly encountered during pregnancy,
with 1 in 500 pregnant women hospitalized for a leiomyoma-related complication.
Approximately half of all leiomyomas grow during pregnancy,
mainly in the first trimester because of rising estrogen levels.
Abdominal pain and uterine contractions can result from necrosis and degeneration of leiomyomas secondary to rapid growth.
Red degeneration is the most common type of degeneration during pregnancy and occurs when a leiomyoma outgrows its blood supply with resulting hemorrhage.
Such leiomyomas can appear on ultrasound as circumscribed masses with cystic spaces or heterogeneous echogenicity.
During pregnancy,
the uterus enlarges and can alter the blood supply to fibroids,
resulting in degeneration.
When this occurs,
patients may present with localized pain,
tenderness,
and fever.
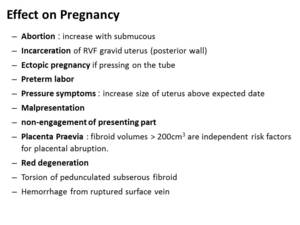
Fig. 10: Effect on pregnancy
References: Clement PB et al.(1992) Am J Surg Pathol 16:26–32.
US
Ultrasound can further confirm a degenerating leiomyoma as the
source of pain if the patient experiences pain when the probe is
directly placed over the leiomyoma.
- concentric,
solid,
hypoechoic masses
- absorb sound waves and therefore cause a variable amount of acoustic shadowing
- Degenerate fibroids may have a complex appearance,
with areas of cystic change. Color doppler typically shows circumferential vascularity
CT
CT scanning also has a limited role in the diagnosis of uterine
fibroids.
On CT scans,
fibroids are usually indistinguishable from healthy
myometrium unless they are calcified or necrotic.
MRI
Leiomyomas with red degeneration may exhibit an unusual signal
intensity pattern at MR imaging:
- Peripheral or diffuse high signal intensity on T1-weighted images
- Variable signal intensity with or without a low-signal-intensity rim on T2-weighted images
- The high signal intensity on T1-weighted images is likely secondary to the proteinaceous content of the blood or the T1-shortening effects of methemoglobin.
- When high signal intensity is isolated to the rim of the leiomyoma,
it has been hypothesized that the blood products are confined to thrombosed vessels that surround the tumor.
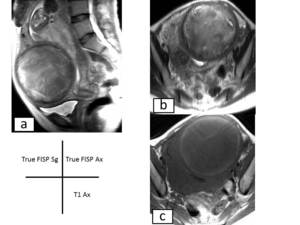
Fig. 11: Degenerating leiomyoma in a 39-year-old pregnant patient at 37 weeks gestation.(a)Sagittal True FISP image and (b)Axial True FISP image, the leiomyoma has high signal intensity due to degeneration.(c)Axial T1-weighted image, the leiomyoma has low signal intensity.
Appendicitis
Appendicitis is the most common nonobstetric reason for emergency surgery during pregnancy,
occurring in approximately 1 in 1,000-1,500 deliveries.
Early diagnosis is important because a 66% increased incidence of appendiceal perforation during pregnancy.
Clinically diagnosing appendicitis duringpregnancy is difficult because of multiple factors including
① The variable appendiceal position
② Limited physical examination of the gravid abdomen
③ The nonspecificity of symptoms such as nausea,
vomiting,
guarding,
and leukocytosis during pregnancy.
US
Ultrasound is usually the first imaging technique of choice.
The sonographic criteria for diagnosing appendicitis in pregnant
patients are the same as in nonpregnant patients.
-wall thickening (> 2 mm)
-appendicoliths
-surrounding hyperechoic inflamed fat
-hypoechoic fluid may also be seen sonographically .
CT
CT is generally performed if MRI is unavailable or if the patient has
contraindications to MRI to prevent a delay in the diagnosis and
treatment of a possible appendicitis.
MRI
―an appendix diameter of > 7 mm with high-T2-signal-intensity
luminal contents
―appendiceal wall thickening (> 2 mm)
―periappendiceal fat stranding and fluid
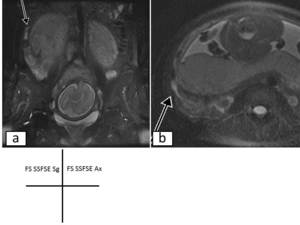
Fig. 12: Acute appendicitis in a 34-year-old pregnant patient at 29 weeks
gestation.(a)Sagittal and(b)Axial fat saturated SSFSE image show a fluid-filled 8-mm-diameter appendix with periappendiceal
inflammatory change. An appendicolith is seen in
the acutely inflamed appendix.
Pancreatitis
Pancreatitis is a rare cause of abdominal pain during pregnancy,
occurring in 0.1–1% of pregnancies and occurring most commonly in the third trimester.
In pregnancy,
gallstones are the most common cause of pancreatitis because pregnancy promotes the formation of sludge and stones within the gallbladder due to increased cholesterol synthesis,
bile stasis,
and decreased gallbladder contraction.
In addition,
higher levels of maternal estrogen in the third trimester can increase triglyceride synthesis and,
in some cases,
can induce pancreatitis secondary to hypertriglyceridemia.
US
Ultrasound is useful to confirm the diagnosis of pancreatitis and to
diagnose gallstone pancreatitis,
while avoiding fetal radiation.
Ultrasound also can be used to detect pancreatic pseudoaneurysms.
CT
Abdominal CT may be indicated when complicated pancreatitis is
suspected.
However,
its routine use in complicated cases should be
avoided because this exposes the fetus to irradiation.
MRI
The peripancreatic fluid and edema associated with pancreatitis
appear as high signal intensity surrounding the pancreas on T2-
weighted images.
Biliary and pancreatic ductal dilatation can also be seen.
Complications of acute pancreatitis that can be seen at MR imaging
include abscess,
pseudocyst,
pancreatic necrosis,
and splenic vein
thrombosis.
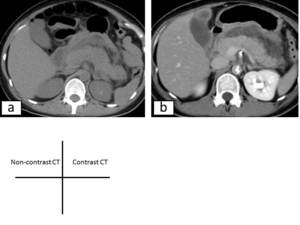
Fig. 13: Acute pancreatitis in a pregnant patient at 36 weeks gestation.a)Unenhanced transverse CT image show a large pancreas.
b)Acute pancreatitis in a pregnant patient after cesarean section. Enhanced transverse CT image show a large, edematous pancreas and peripancreatic inflammatory changes.


Sagittal T2-weighted SSFSE image shows the uterus maintains its normal version and flexion.(b)Sagittal T2-weighted SSFSE image shows the gravid uterus increases in size and displaces the pelvic contents from their normal locations.")
Oblique T2-weighted image,(b)Fat saturated Contrast-enhanced T1-weighted image,(c)Sagittal T2-weighted image shows eccentric intrauterine gestational sac that is not surrounded by endometrium.")
Axial T1-weighted image,b)Axial Fat saturated contrast-enhanced T1-weighted image,c)Coronal true FISP image show a right ovarian mass that contains fat and fluid.
On the fat-saturated image, note the loss of the high signal
intensity in the macroscopic fat component of the mass.")
Sagittal True FISP image and (b)Axial True FISP image, the leiomyoma has high signal intensity due to degeneration.(c)Axial T1-weighted image, the leiomyoma has low signal intensity.")
Sagittal and(b)Axial fat saturated SSFSE image show a fluid-filled 8-mm-diameter appendix with periappendiceal
inflammatory change. An appendicolith is seen in
the acutely inflamed appendix.")
Unenhanced transverse CT image show a large pancreas.
b)Acute pancreatitis in a pregnant patient after cesarean section. Enhanced transverse CT image show a large, edematous pancreas and peripancreatic inflammatory changes.")