ECR 2013 / C-1216
Radiological assessment of skull sutures in Patients with syndromic craniosynostosis.
Congress:
ECR 2013
Poster Number:
C-1216
Type:
Educational Exhibit
Keywords:
Anatomy, Neuroradiology brain, Paediatric, CT-High Resolution, MR, CT, Computer Applications-3D, Computer Applications-Detection, diagnosis, Computer Applications-General, Cerebrospinal fluid, Congenital, Image verification
Authors:
G. D'Apolito, R. Calandrelli, G. Di Lella, A. M. Costantini, C. Colosimo; Rome/IT
DOI:
10.1594/ecr2013/C-1216

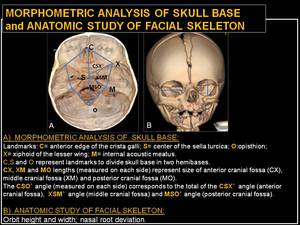
Fig. 12:
Morphometric analysis of skull base and anatomic study of facial skeleton.
: symmetry preserved. References: Department of Bio-imaging and Radiological Sciences, Catholic University of Rome - Rome/IT")
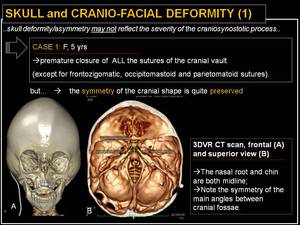
Fig. 13:
Skull and cranio-facial deformity (1): symmetry preserved.
: symmetry not preserved. References: Department of Bio-imaging and Radiological Sciences, Catholic University of Rome - Rome/IT")
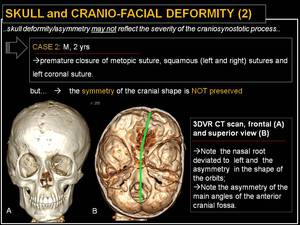
Fig. 14:
Skull and cranio-facial deformity (2): symmetry not preserved.
: unilateral coronal synostosis. References: Department of Bio-imaging and Radiological Sciences, Catholic University of Rome - Rome/IT")
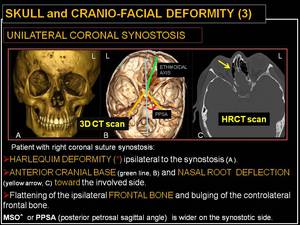
Fig. 15:
Skull and cranio-facial deformity (3): unilateral coronal synostosis.
: unilateral frontosphenoidal synostosis. References: Department of Bio-imaging and Radiological Sciences, Catholic University of Rome - Rome/IT")
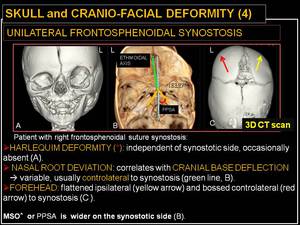
Fig. 16:
Skull and cranio-facial deformity (4): unilateral frontosphenoidal synostosis.
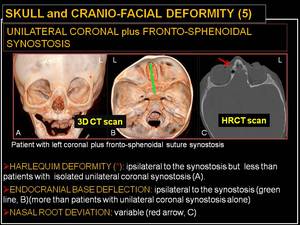
: unilateral coronal and frontosphenoidal synostosis. References: Department of Bio-imaging and Radiological Sciences, Catholic University of Rome - Rome/IT")
Fig. 17:
Skull and cranio-facial deformity (5): unilateral coronal and frontosphenoidal...

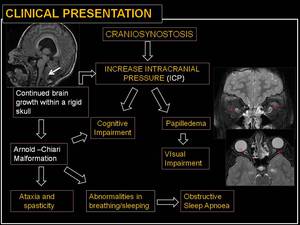
Fig. 18:
Clinical presentation.
. References: Department of Bio-imaging and Radiological Sciences, Catholic University of Rome - Rome/IT")
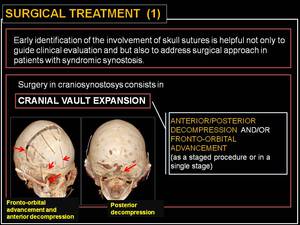
Fig. 19:
Surgical treatment (1).
. References: Department of Bio-imaging and Radiological Sciences, Catholic University of Rome - Rome/IT")
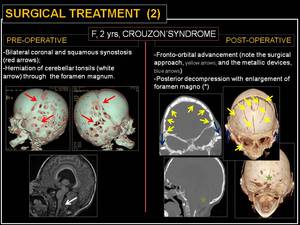
Fig. 20:
Surgical treatment (2).