Localization of the lesions
To make a correct localization of the lesions we should know the different spaces and limits,
which compose the retroperitoneum.
This anatomic space is delimited Fig. 2 superiorly by the diaphragm,
lower limit: the pelvis,
anterior : posterior parietal peritoneum and posterior by transversalis fascia.
The retroperitoneum almost its divided in different areas: posterior pararenal space,
anterior pararenal space,
perirenal space and space of the great vessels.
One of the challenges to radiologist its the correct localization of the retroperitoneal lesions and the characterization and in the assessment of the extent of the disease and involvement of adjacent structures,
identifying the organ of origin,
to these purpose we use different radiologic signs (6):
- Beak Sign : When the border of the affected organ its deformed like a ¨beak¨ (acute angle) should be considered that the lesion or tumor arises from there.
If the margins of the organ which is in contact presents a blunt edge,
the lesion is shifting the organ.
- Embedded organ sign (positive or negative): When the border adopts a crescent shape morphology in plastic organs correspond that these lesion doesn’t depends from this organ,
because the organ is displace for these lesion,
if the structure is fused with the surface of the lesion (embedded organ sign),
indicate invasion or you can conclude that this tumor arise from this structure.

Fig. 1: Nishino M, Hayakawa K, Minami M. Primary retroperitoneal neoplasm: CT and MR imaging findings with anatomic and pathologic diagnostic clues. Radiographic 2003;23:45.
References: Nishino M, Hayakawa K, Minami M. Primary retroperitoneal neoplasm: CT and MR imaging findings with anatomic and pathologic diagnostic clues. Radiographic 2003;23:45.
The pathologies of the retroperitoneum can be divided into neoplastic and non-neoplastic lesions.
The non-neoplastic pathologies are hematomas and urinomas usually secondary to traumas,
abscessed collections and inflammatory diseases.
- No Neoplastic Lesions
Hematomas
The formation of hematomas is usually secondary to trauma and less frequently to blood dyscrasias or use of anticoagulants Fig. 3 Acute and subacute hematomas have a heterogeneous attenuation and morphology on CT.
At MR imaging hematomas demonstrates high signal intensity on T1-weighted images (2).
Chronic hematoma shows fluid attenuation by CT and may be difficult to distinguish from abscesses and cystic tumors,
percutaneous aspiration may be useful to differentiate between these etiologies.
The MR imaging appearance of hemorrhage depends on the age of the hematoma in chronic hematomas produces areas of low signal intensity on both nonenhanced T1- and T2-weighted images.
Urinomas
They are encapsulated collections of extravasated urine to the retroperitoneal space most commonly secondary to trauma,
manipulation of the urinary tract,
surgery and less common from obstructive uropathy.
The most frequently localization of the urinomas are perirenal space,
CT shows a well-defined hipointense fluid collection,
studies with intravenous contrast material shows the increase of the attenuation in delayed phase images of the urinoma over time.
On a T2-weighted MR urinomas usually shows a well-defined surface,
homogeneous high signal intensity in retroperitoneal space
Retroperitoneal Fibrosis
Retroperitoneal fibrosis is an uncommon disease that affects the connective tissue of the retroperitoneum space,
is more prevalent in women than in men (3:1) 5th and 6th decade,
and 70% of cases are idiopathic and the remainder is associated with fibrosing diseases suggesting auto-immune mechanism such as sclerosing cholangitis,
glomerulonephritis,
fibrosing mediastinitis,
fibrotic pseudotumor of the orbit,
thyroiditis,
systemic lupus erythematosus (SLE) and autoimmune pancreatitis,
other related causes are infections conditions,
radiation,
chemotherapy,
drugs and bleeding.
Fig. 4
On unenhanced CT the retroperitoneal fibrosis presents as a plaque or mass of soft tissue isodense with the muscle around the aorta and inferior vena cava,
between the kidney and sacrum.
Retroperitoneal fat changes are more frequent in the infrarenal aorta and iliac arteries,
affecting all retroperitoneal structures Fig. 4.

Fig. 4: Contrast enhanced CT reveals a retroperitoneal mass surrounding the great vessels space (predomly left), that mass produce obstruction of urinary tract with bilateral hydronefrosis. Hystopatologic study confirms retroperitonal fibrosis.
Retroperitoneal fibrosis doesn’t produce an anterior displacement of the aorta in contrast to lymphoma and metastases,
surrounding to involve the ureters,
causing varying degrees of urinary obstruction.
After de intravenous contrast retroperitoneal fibrosis present an enhancement in acute episode and low enhancement or absence in the chronic stages.
MR imaging shows high signal intensity on T2-weighted images in the acute phase of
the disease,
with early contrast enhancement and low signal intensity on T2 (dense fibrotic stage).
2.
Neoplastic More Frequent
Such are the most common neoplasms in the retroperitoneum approximately 33% and represent between 3% - 8% of patients who require staging of non-Hodgkin lymphoma (1) at initial stage at diagnosis Fig. 6 ,
Retroperitoneal lymphomas may present with multiple homogeneous masses or as a mass in the perirenal space.
These lesions involve the great vessels or can produce an anterior displace of the kidneys including their hila without invasion.
One of the most common complications in lymphomas are the ureteral obstruction,
with hidronefrosis.
CT scan shows a mass with well-defined borders,
with mild homogeneous enhancement after intravenous contrast, that spreads between normal structures without compressing them,
great vessel specially aorta can be displaced anteriorly.
MR imaging of the lymphomas shows an heterogeneous signal,
been isointense at T1-weighted images,
in T2-weighted sequences,
lesions shows iso-hiperintense signal.

Fig. 7: CT study showing grouped well defined nodular lesions in the retroperitoneal region, surrounding both renal hila.
The teratomas are neoformative proceses that arise from aberrant primordial germ cell rests that are due tofaulty migration of germ cells from the yolk sac or endoderm to the urogenital.
These kinds of tumors are infrequent at the retroperitoneum,
with report series less than 10 % of all teratomas,
and less than 11 % of all the primary retroperitoneal primary pathologies,
been more frequent in pediatric patients Fig. 8
Teratomas are compose for different kind of well differentiated tissues at least two germ cells.
The most frequent characteristic of the termatomas are the presence of calcifications an adipose tissue inside de lesion Fig. 9 been solid and less frequent cystic.
Malignant teratomas present a irregular morphology and important infiltration of adjacent structures.
Neoformative procces derived from sympathetic ganglion cells,
its more frequent in pediatric patients.
This tumors presents a heterogeneous morphology related with intralesion bleeding or necrotic areas secondary to the large size that can adopt. Fig. 10
The principal metastasis of these tumors are local invasion in less differentiate tumors.
- Neoplasms derived from mesoderm
Most of the neoplasms that arise in the retroperitoneum derivates from mesodermic cells are malignant,
that kind of tumors presents a frequency of approximately 80% within the most frequently observed are leiomyosarcoma Fig. 11 ,
liposarcoma,
and others undifferentiated sarcomas.

Fig. 11: Neuroblastoma affects retroperitoneum in a patient of 8 years old. T2-weighted MR imaging shows a well-defined heterogeneous mass, with heterogeneous signal and displace anteriorly the adjacent structures
Most of the sarcomas are observed between the fifth and sixth decades of life,
as most of the retroperitoneal pathologies may have a slow clinical evolution,
that it’s the principal reason that the sintoms are usually in tumors with large sizes,
displacing or invading adjacent structures in the retroperitoneum.
Sarcomas have a high rate of recurrence and metastases often to liver,
lung and bone.
It is the most common malignancy of retroperitoneal sarcomas corresponding approximately 30%,
the age of frequency are between 5 and 7 decade. Fig. 13
Liposarcomas are divided in four subtypes,
well-differentiated,
myxoid,
round cell and pleomorphic,
all related with diferents grades of malignancy.
In imaging studies ,
liposarcomas are hypodense on CT because of its high content fat,
on MRI presents a high signal at T1-weighted images,
intermediate-signal in T2-weighted sequences,
and a drop signal in fat suppression sequences .
Represents approximately 29% (1) of the retroperitoneal tumors originating in the mesoderm,
is most common between the 4 and 6 decades of life.
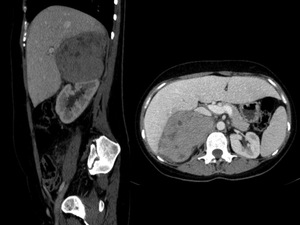
Fig. 14: Abdominal CT enhanced show a heterogeneous retroperitoneal lesion, displacing inferiorly the right kidney. Hystologic study reveals leiomiosarcoma.
The leiomiosarcamosa originate mainly in the retroperitoneal connective tissue,
blood vessels and less frequently in the remnants of the Wolffian ducts.
By location grow to a great size greater than 10 cm.
In the CT study shows a heterogeneous retroperitoneal mass with necrosis areas.
The MRI shows a heterogeneous mass with a low or intermediate signal on T1-weighted sequences and high signal on T2,
the presence of lesions with large areas of necrosis surrounded by vessels is highly suggestive of leiomyosarcoma.



 that affects perirenal space and pararenal space, after 3 minutes of contrast the hematoma presents extravased contrast in relation with active bleeding.")
, that mass produce obstruction of urinary tract with bilateral hydronefrosis. Hystopatologic study confirms retroperitonal fibrosis.")
.")
")




 shows a retroperitoneal solid lesion with well-defined borders, surrounding aorta and occludes the right ureter hydronephrosis conditioning. MRI study (2) spin-eco T2-weighted shows para-aortic lesion visualized on CT in relation to sarcomatous process")

