ECR 2013 / C-1343
Splenic Cystic Lesions – Differential Diagnosis
Congress:
ECR 2013
Poster Number:
C-1343
Type:
Educational Exhibit
Keywords:
Abdomen, Spleen, CT, Ultrasound, Diagnostic procedure, Cysts, Neoplasia, Abscess
Authors:
N. Neto1, P. G. M. G. Ferreira2, A. Vasconcelos3; 1Lisbon/PT, 2Amadora/PT, 3Barreiro/PT
DOI:
10.1594/ecr2013/C-1343
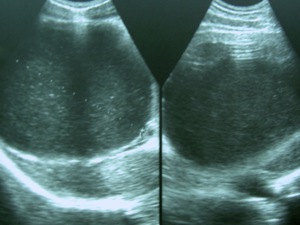
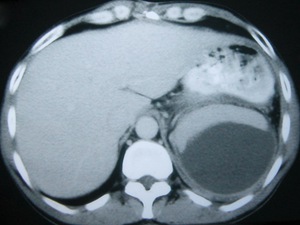
 cystic unilocular mass, with non-pure content.")
Fig. 1:
US scan of a patient, who presented with left upper quadrant pain, revealed a...

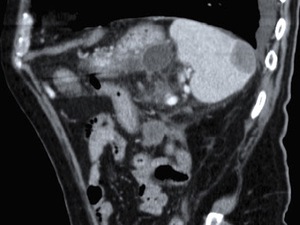
Fig. 2:
Unenhanced CT scan of the same patient as in figure 1, confirmed the...

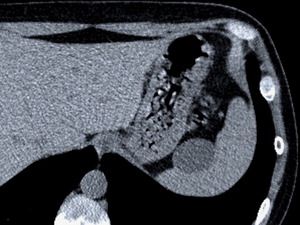
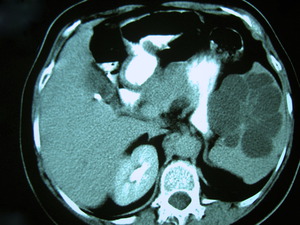
Fig. 3:
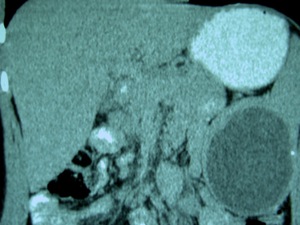
Contrast-enhanced CT scan of a patient, who had had an acute pancreatitis...

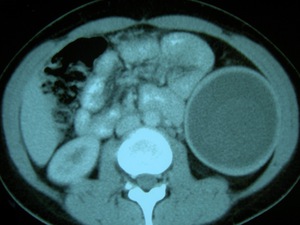
Fig. 4:
Another “false” cyst detected in a patient who had had a blunt abdominal...

Fig. 5:
Primary splenic hydatidosis in a 24-year-old woman, who underwent imaging...

Fig. 6:
The same lesion as in figure 5 at contrast-enhanced CT, appeared as a...

Fig. 7:
Note the incipient calcification of the hydatid cyst’s wall described in...

Fig. 8:
The spleen of a septic patient replaced by a low-attenuation and slightly...
 and splenomegaly. Contrast-enhanced CT revealed a nonenhancing hypodense area, wedge-shaped and of fluid attenuation in its left portion, representing hemorrhagic necrotic tissue.")
Fig. 9:
Splenic infarct in a 56-year-old patient with chronic hepatic disease (CHD) and...

Fig. 10:
Note the subcapsular fluid-fluid level in the inferior half of the spleen,...

Fig. 11:
Splenic subcapsular hematoma after a blunt abdominal trauma. Contrast-enhanced...

Fig. 12:
Splenic hemangioma incidentally detected at an US scan in an asymptomatic...

Fig. 13:
A contrast-enhanced CT scan of the same patient as in figure 13, showed the...

Fig. 14:
Marginal zone B-cell non-Hodgkin lymphoma in a 71-year-old man, who underwent...

Fig. 15:
Multiple splenic cystic metastases of breast adenocarcinoma in a 87-year-old...

Fig. 16:
A coronal slice of the same CT scan as in figure 16, shows how numerous the...

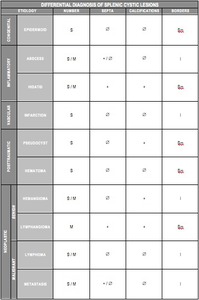
Table 1:
Main characteristic imaging features of splenic cystic lesions, according to...