ECR 2013 / C-1554
MENINGIOMAS: Imaging findings and interpretative pitfalls
Congress:
ECR 2013
Poster Number:
C-1554
Type:
Educational Exhibit
Keywords:
Neoplasia, Education and training, Education, Diagnostic procedure, MR, CT, Catheter arteriography, Neuroradiology brain
Authors:
V. Mayoral Campos1, M. J. Gimeno Peribáñez1, J. A. Guirola2, C. Bonnet Carron1, J. I. Pina Leita1, R. Lasierra Diaz1; 1Zaragoza/ES, 2ZARAGOZA, ZA/ES
DOI:
10.1594/ecr2013/C-1554

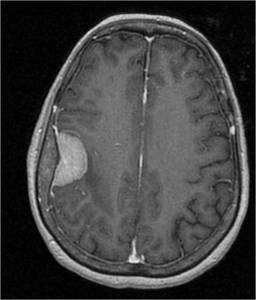
Fig. 1:
The cleft sign: thin rim of CSF surrounding this large meningioma
 References: Department of Radiology, Hospital Clinico Lozano Blesa. Zaragoza/Spain 2012")
Fig. 2:
The subarachnoid vessels that run on the surface of the brain are displaced by...

Fig. 3:
Axial enhanced T1WI. Meningioma with dural tail, hyperostosis and enhancement...

Fig. 5:
Axial CT-scan: bone hyperostosis

Fig. 6:
Axial unenahnced and contrast enhanced CT scan show a large occipital...

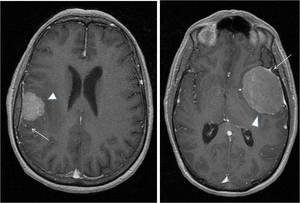
Fig. 7:
Axial unenhanced and enhanced CT scan: extra-axial lesion, hyperintense to...
 and parenchimal edema sourrounding the lesion (short arrows) in two patient with meningiomas. References: Department of Radiology, Hospital Clinico Lozano Blesa. Zaragoza/Spain 2012")
Fig. 8:
Pattern of calcification (long arrow) and parenchimal edema sourrounding the...

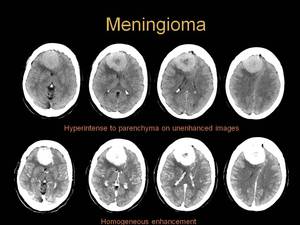
Fig. 9:
CT characteristics of meningioma

Fig. 10:
Sagital T1-weighted spin-eco MR image of the brain shows a large lesion that is...

Fig. 11:
Axial T2-weighted spin-eco MR image of the brain shows a large lesion that is...

Fig. 12:
Axial T1-weighted and T2-weighted MR images show a right parietal mass
that...

Fig. 13:
Inversion recovery sequences demostrating parenchimal edema sourrounding the...

Fig. 14:
With the administration of gadolinium, MR enhanced images demonstrate markedly...

Fig. 16:
Mother in law sign: Common carotid artery injection during the venous phase...
 Axial unenhaced CT-scan shows an extra-axial lesion, hyperintense to parenchyma and with central and peripheral calcification.
b) Axial contrast enhanced CT-scan demostrate not important changes respect unhenanced CT scan.This is not the normal behaviour of a meningioma neither a permeable aneurysm. References: Department of Radiology, Hospital Clinico Lozano Blesa. Zaragoza/Spain 2012")
Fig. 17:
CASE 1
a) Axial unenhaced CT-scan shows an extra-axial lesion, hyperintense to...
 References: Department of Radiology, Hospital Clinico Lozano Blesa. Zaragoza/Spain 2012")
Fig. 18:
Sagital T1, DP, Axial T2 and angio RMI 3D TOFF show a mass with vascular...
")
Fig. 19:
The angiography demostrates an aneurysm in the left ophtalmic-carotid artery...
. It has homogeneous enhancement with contrast medium administration. This is highly suggestive of meningioma References: Department of Radiology, HCU Lozano Blesa, Zaragoza/Spain 2013")
Fig. 20:
CASE 2
Axial unenhanced and enhanced CT scan show a small hyperdense mass near...
 T2-weighted axial spin-eco MR image of the brain shows an isointense mass related to the lesser wing of the sphenoid.
b)T1-weighted axial spin-eco MR image after the administartion of gadolinium demostrate markedly homogeneous enhancement of the mass.
This two findings are highly suggestive of meningioma.
(Same patient figure 20) References: Department of Radiology, Hospital Clinico Lozano Blesa. Zaragoza/Spain 2012")
Fig. 21:
a) T2-weighted axial spin-eco MR image of the brain shows an isointense mass...

Fig. 22:
CASE 3
Sometimes it is difficult to differenciate extra-axial versus...
 T1-weighted coronal spin-eco MR shows an hyperintense lesion that seems to depend on sphenoid. B) T1-weighted coronal and sagittal spin-eco MR demostrate that the lesion is a pituitary macroadenoma. References: Department of Radiology, HCU Lozano Blesa, Zaragoza/Spain, 2013")
Fig. 23:
CASE 4
A) T1-weighted coronal spin-eco MR shows an hyperintense lesion that...