ECR 2013 / C-1881
Strategy and clinical results of uterine fibroid embolization (UFE) for symptomatic uterine leiomyoma patients: analysis of over nine hundred cases
Congress:
ECR 2013
Poster Number:
C-1881
Type:
Educational Exhibit
Keywords:
Interventional vascular, Catheter arteriography, Embolisation, Outcomes
Authors:
K. Koyama1, S. Yagi2, T. Fukushita2, H. Fujisawa3, T. Kushihashi3, Y. Taki4, T. Kojima2; 1Yokohama, Kanagawa/JP, 2Yokohama/JP, 3Kanagawa/JP, 4Tokyo/JP
DOI:
10.1594/ecr2013/C-1881

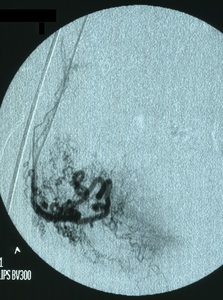
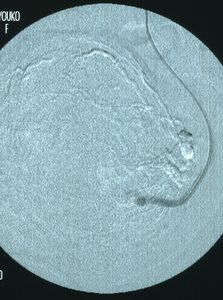
Fig. 1:
Angiography of the right uterine artery

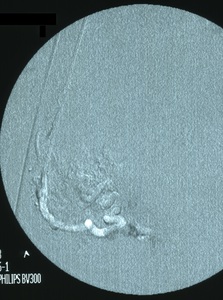
Fig. 2:
Angiography of the right uterine artery

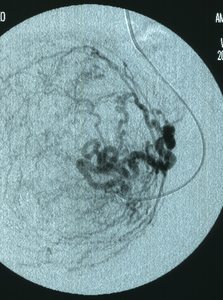
Fig. 3:
Angiography of the left uterine artery

Fig. 4:
Angiography of the left uterine artery

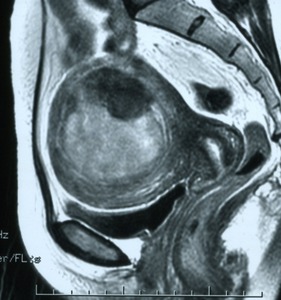
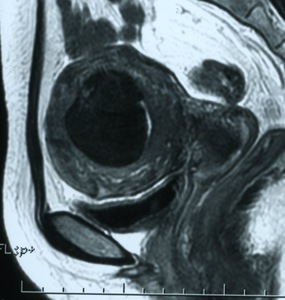
Fig. 5:
MR T2-weighted image of the uterine leiomyoma before UFE

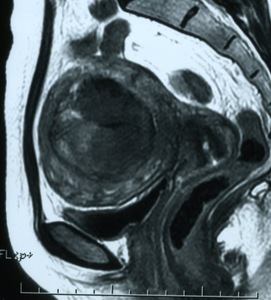
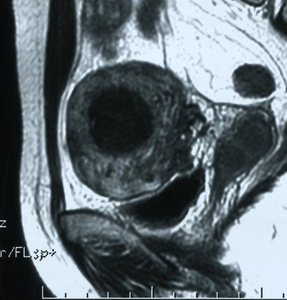
Fig. 6:
MR T2-weighted image of the uterine leiomyoma after UAE 1 month

Fig. 7:
MR T2-weighted image of the uterine leiomyoma after UAE 3 months

Fig. 8:
MR T2-weighted image of the uterine leiomyoma after UAE 6 months

Fig. 9:
MR T2-weighted image of the uterine leiomyoma after UAE 1 year