Renal transplantation from a living donor or cadaver represents currently the treatment of choice for patients with chronic renal failure in terminal uremic stage; despite the recent progress obtained in terms of survival with hemodialysis and peritoneal dialysis,
transplantation is the best treatment not only to restore a normal kidney function,
but also to propose a good quality of life in most cases.
Careful donor selection and an accurate study of recipients are crucial for the transplantation.
In addition,
it is easy to understand the importance of monitoring the post-transplant course,
in order to identify early any post-operative problems [1].
Renal transplantation techniques
We illustrate the different surgical techniques of renal transplantation:
- Monolateral single kidney transplantation;
- Bilateral dual kidney transplantation / monolateral dual kidney transplantation;
- Joined monolateral dual kidney transplantation.
The knowledge of these surgical techniques allows radiologists to easily identify the renal complications.
1.
Monolateral single kidney transplantation.
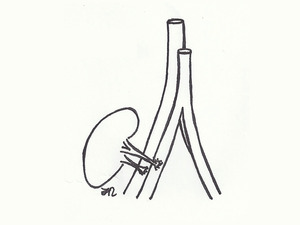
Fig. 1: Monolateral single kidney transplantation: vascular anastomoses are performed using the right external iliac artery and the right external iliac vein.
There are 3 possibilities of placement for renal graft: extra-peritoneal,
trans-peritoneal and intra-peritoneal.
In heterotopic renal transplantation,
the renal graft is implanted in the right iliac fossa; the right iliac fossa is preferred because exposure of the iliac vessels is greater than in the left iliac fossa.
Extra-peritoneal placement of the renal graft into iliac fossa provides the following advantages:
- Wide adaptability of renal graft;
- Availability of iliac vessels for the anastomoses (iliac vessels are similar in size to the renal arteries and veins)
- Low infection potential;
- Short distance to the bladder (allowing to mobilize the distal end of the ureter for the anastomosis with the bladder);
- Evaluation of renal graft dysfunction.
In most cases,
the vascular anastomoses are performed using the right external iliac artery and the right external iliac vein [2,3].
The most common technique is the end-to-side anastomosis between the renal artery of the neo-kidney and the external iliac artery.
The venous anastomosis is performed between the renal graft vein and the right external iliac vein (end-to-side anastomosis); the left kidney is preferred for donation because the vein is longer; if renal veins are excessively short,
it is possible to use a vein patch [4].
The most common surgical procedure for ureteral implantation is the “Politano-Ledbetter reformatting technique”,
also called intra-bladder anastomosis: in this surgical procedure,
a short sub-mucosal tunnel in the trigonal region is performed,
in order to create an anti-reflux mechanism.
2 Bilateral dual kidney transplantation / Monolateral dual kidney transplantation
In recent years criteria for organ procurement have been changed,
and a significant role has been attributed to older donors and dual kidney transplantation.
Due to the disparity between organ supply and demand,
the use of “expanded donor criteria” has been accepted: kidneys of elderly subjects,
with limited potential,
are transplanted in a single receiver in order to increase the nephronic mass and improve the long-term survival of these "marginal” transplants [5].
The choice of surgical technique is critical since the potential disadvantages of DKT,
due to the longer operative times and percentage of risks increased when compared to "standard" monolateral single kidney transplant.
The kidneys could be implanted with two Gibson incisions (less frequently using a single medial incision); alternatively,
a single Gibson incision has been used to place both renal grafts in an extra-peritoneal location (unilateral dual kidney transplantation,
UDKT) [5].
The most commonly used technique for bilateral dual kidney transplantation has been introduced by Masson and Hefty; the right kidney is implanted performing venous anastomosis to the vena cava and arterial anastomosis to the right external iliac artery; the left kidney is anastomosed to the right external iliac vein and to the common iliac artery.
In the monolateral dual kidney transplantation,
the arteries and veins of the two monolateral kidneys are anastomosed into the external iliac vessels.
4.
Joined monolateral dual kidney transplantation.
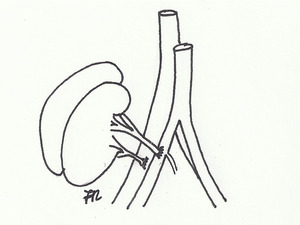
Fig. 2: Joined monolateral dual kidney transplantation: the arteries and veins of the two monolateral kidneys are joined thorough a running suture (unilateral fusion of vessels), and the joined kidneys are anastomosed into the external iliac vessels.
Dual Kidney Transplantation (DKT) might be considered a major surgical procedure and,
in older recipients,
has a potentially greater risk of surgical complications compared with the single kidney transplantation.
The monolateral dual kidney transplantation has been adopted to reduce these surgical complications.
Some Authors introduced a new technique called joined monolateral dual kidney transplantation [6]: the arteries and veins of the two monolateral kidneys are joined thorough a running suture (unilateral fusion of vessels),
and the joined kidneys are anastomosed into the external iliac vessels.


, and the joined kidneys are anastomosed into the external iliac vessels.")