Materials:
This retrospective study involved a group of 19 patients hospitalized in SP CSK im.
prof.
K.
Gibińskiego SUM in Katowice,
who in 2005-2012 were treated with targeted thrombolysis and mechanical thrombectomy.
The average age of patients with ischemic stroke was 60.36 years (with a range of 26-84 years) (Table 1).
Neurological examination (assessed using the National Institutes of Health Stroke Scale [NIHSS]) was performed before and after surgery and at discharge from the ward.
Table 1
References: Student Scientific Society of Interventional Radiology, Medical University of Silesia/ Katowice 2013
Qualifications protocol:
In order to exclude patients with hemorrhagic stroke,
procedures (CT,
Angio-CT and/or DSA angiography) were performed at the start of diagnosis (Fig.
1).
If vascular changes were visualized,
a procedure was applied according to the following scheme.
A significant role in the treatment of stroke plays the start time of therapy aiming at streamlining vessels.
However,
the method thrombolysis i.v.
can be applied only to the 4.5 hours after the first symptoms,
which includes only 5% of patients.
Thrombolysis i.a.
(targeted) is an endovascular procedure of treating recent arterial thrombosis with the use of fibrinolytics: urokinase,
recombinant tissue plasminogen activator (r-tPA) or streptokinase.
It can be applied in selected patients with large stroke up to 6 hours after the onset of symptoms and/ or a contraindication to the use of thrombolysis i.v..
For several years,
the method of mechanical thrombectomy is used.
This method consists in introduction of catheter into cerebral vessels that allow the mechanical removal of the embolism.
They extend the therapeutic window for patients with large stroke up to 8 hours from onset of symptoms and/ or contraindicated or inefficient iv thrombolysis,
which significantly increases the number of patients eligible for treating.
This type of equipment includes a Penumbra set which uses a guidewire and a separator for mechanical thrombus fragmentation.
A high rate of recanalization and a favorable clinical outcome in patients with occlusion of proximal parts of arteries can be achieved with a Solitaire stent.
Clinical effects and the outcome of treatment depend mostly on the initial neurological status and the time in which treatment begins.
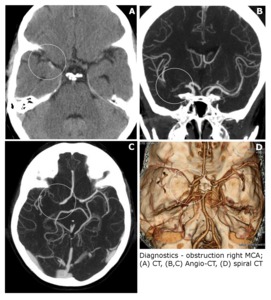
Fig. 1
References: Student Scientific Society of Interventional Radiology, Medical University of Silesia/ Katowice 2013
Targeted thrombolysis:
All procedures were performed with the initial puncture of the right femoral artery and introducing the catheter using the Seldinger method.
A contrast agent was then administered to visualize the obstruction of the cerebral vessels.
The diagnostic catheter was later replaced by a leading catheter and a coaxially introduced guidewire whose end was placed in the occluded vessel.
Finally a 10 to 20 ml dose of r-tPA was given.
During the procedure continuous rinsing,
using a heparin solution in saline,
of both the guiding catheter and the guidewire,
was performed (Fig.
2).
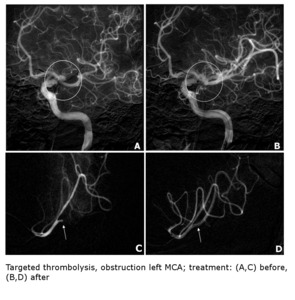
Fig. 2
References: Student Scientific Society of Interventional Radiology, Medical University of Silesia/ Katowice 2013
Mechanical thrombectomy:
The procedure was performed with the initial puncture of the right femoral artery and introducing the catheter using the Seldinger method.
The guidewire of the Penumbra system for mechanical thrombectomy was then coaxially introduced and aspiration of the thrombus was performed.
The aspiration catheter was placed below the thrombus and the separator was introduced into the center of the thrombus (Fig.
3).
After connecting suction,
the seperator broke up the thrombus and the fragments were aspired.
When using the Solitaire stent,
it was depressurized above the thrombus without complete release.
The thrombus was then pulled through the leading catheter.
During the procedure rinsing with heparin solution in saline,
of both the guiding catheter and the guidewire,
was performed (Fig. 4).
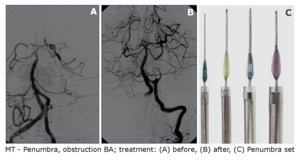
Fig. 3
References: Student Scientific Society of Interventional Radiology, Medical University of Silesia/ Katowice 2013
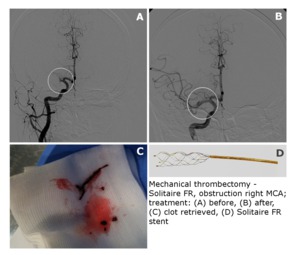
Fig. 4
References: Student Scientific Society of Interventional Radiology, Medical University of Silesia/ Katowice 2013
Classification TICI:
The success of recanalization and reperfusion have been evaluated using TICI scale with assigning five classification degrees (Table 2).
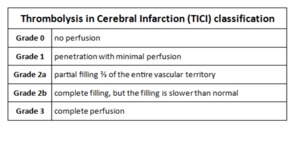
Table 2
References: Student Scientific Society of Interventional Radiology, Medical University of Silesia/ Katowice 2013
Control after intervention:
After the procedure were performed CT and DSA angiography in order to assess patency and exclude intracranial hemorrhage (Fig. 5).
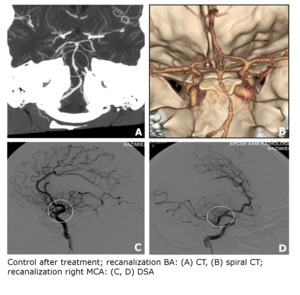
Fig. 5
References: Student Scientific Society of Interventional Radiology, Medical University of Silesia/ Katowice 2013







