ECR 2013 / C-2085
Methods for endovascular treatment of cerebral vascular obstruction - own experience
Congress:
ECR 2013
Poster Number:
C-2085
Type:
Scientific Exhibit
Keywords:
Neuroradiology brain, Interventional vascular, Catheter arteriography, Thrombolysis, Recanalisation, Catheters, Obstruction / Occlusion, Embolism / Thrombosis, Ischaemia / Infarction
Authors:
M. Honkowicz1, T. Kirmes2, M. Koronski3, M. Kysiak4, M. Bukanski5, D. T. Knap6, D. Sieron6, J. Baron6; 1Gorlice/PL, 2Tychy/PL, 3Nowy Sacz/PL, 4Stryszawa/PL, 5Kuznia Raciborska/PL, 6Katowice/PL
DOI:
10.1594/ecr2013/C-2085

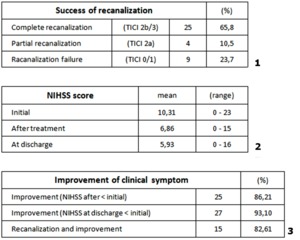
Table 3

Table 4

Table 5

Table 6