ECR 2013 / C-2096
ARTICULAR CAUSES OF HIP PAIN: NEW and ANCIENT CONCEPTS
Congress:
ECR 2013
Poster Number:
C-2096
Type:
Educational Exhibit
Keywords:
Musculoskeletal bone, Musculoskeletal system, Anatomy, CT, MR, Arthrography, Acute, Arthritides, Developmental disease
Authors:
V. Mascarenhas, F. Morais, P. D. Afonso, A. Guerra, H. M. R. Marques, A. M. Gaspar; Lisbon/PT
DOI:
10.1594/ecr2013/C-2096
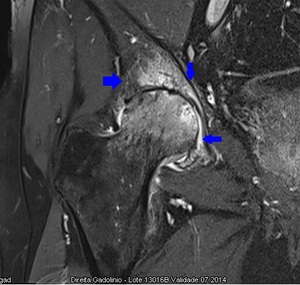
. Capsular thickening (green arrowhead) and CAM-deformity with increased alpha angle(blue arrowhead). References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
Fig. 5:
Radial PD WI of the right hip (arthro-MRI). Capsular thickening (green...
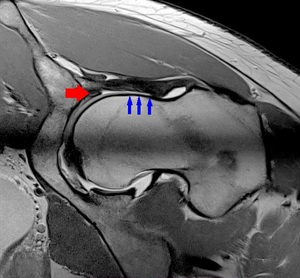
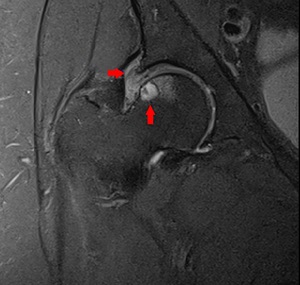
. Increased alpha angle, labral degeneration (red arrowhead) and CAM-deformity (blue arrowhead). References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
Fig. 6:
Radial PD WI of the left hip (arthro-MR). Increased alpha angle, labral...
. Increased acetabular coverage (blue arrowhead) and infra-cervical plicae are noted (red arrowhead). References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
Fig. 7:
Coronal PD WI of the right hip (arthro-MRI). Increased acetabular coverage...
. Increased acetabular coverage (blue arrowhead) and hypertrophic labrum (red circle). References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
Fig. 8:
Coronal PD WI of the left hip (arthro-MRI). Increased acetabular coverage (blue...
. Synovial herniation pit (red circle). References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
Fig. 9:
Radial PD WI of the right hip (arthro-MRI). Synovial herniation pit (red...
. Full-thickness focal acetabular chondral lesion. References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
Fig. 10:
Coronal PD WI of the left hip (arthro-MRI). Full-thickness focal acetabular...
. Intra-substance degeneration of the Labrum. References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
Fig. 11:
Radial PD WI of the left hip (arthro-MRI). Intra-substance degeneration of the...
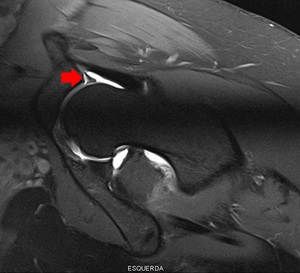
. Rupture of the labral base. References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
Fig. 12:
Radial PD Fat-Sat WI of the left hip (arthro-MRI). Rupture of the labral base.
, short and thick neck of femur (blue arrowhead). References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
Fig. 13:
CR of the left hip. Achondroplasia with coxa vara (angle red lines), short and...
. References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
Fig. 14:
CR of the lower limbs. Achondroplasia with bilateral coxa vara (angle red...
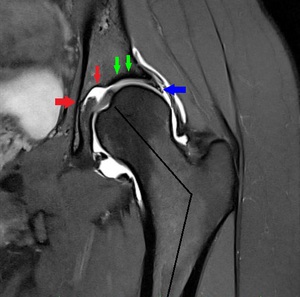
. Acetabular dysplasia (green arrowhead) with fovea Alta (red arrowhead), coxa valga (angle black lines) and hypertrophic labrum(blue arrowhead). References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
Fig. 15:
Coronal PD Fat-Sat WI of the left hip (arthro-MRI). Acetabular dysplasia (green...
 with coxa valga (angle red lines). References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
Fig. 16:
CR of the left hip. Deep acetabulum coxa profunda (blue arrowhead) with coxa...

Fig. 17:
CR of the pelvis. Tonnis grade 2 changes of the right hip.

Fig. 18:
Sagital PD Fat-Sat WI of the right hip. Multiple subchondral cysts in a...
. References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
Fig. 3:
3D CT reformats of the right hip. Huge dense lesion with articular destruction...
and CAM deformity (blue arrowhead). References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
Fig. 19:
Radial PD WI of the right hip. Osteophytes, chondral lesions (red arrowhead)and...

Fig. 20:
Coronal PD WI of the right hip. Linear irregularity of the femoral epiphysis...

Fig. 21:
CR of the pelvis. Bilateral irregularity of the femoral epiphyseal regions with...

Fig. 22:
Coronal PD WI left hip. Irregularity of the femoral epiphyseal region with...

Fig. 23:
Coronal PD WI of the right hip. Protrusio acetabuli with multiple tiny erosions...

Fig. 24:
Coronal T1 FS WI GAD of the right hip. Marked enhancement of both articular...

Fig. 25:
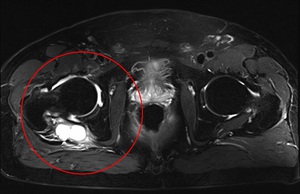
Axial T2 Fat-Sat WI of the pelvis. Psoriatic arthritis with huge peri-articular...

Fig. 26:
Axial T1 Fat-Sat WI GAD of the right hip. Psoriatic arthritis with huge...

Fig. 27:
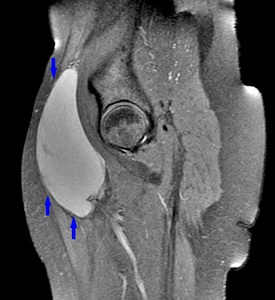
Axial T2 Fat-Sat WI of the right hip. Persistent articular effusion following...

Fig. 28:
Coronal T2 WI of the right hip. Persistent Articular effusion following...

Fig. 29:
CR of the right hip. Osteomyelitis. Huge dense lesion with articular...
. Osteomyelitis. Huge dense lesion with articular destruction. References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
Fig. 30:
CT of the right hip (coronal reformat). Osteomyelitis. Huge dense lesion with...

Fig. 31:
Coronal PD Fat-Sat WI of the right hip. Multiple tiny intra-articular bodies of...

Fig. 32:
Sagital PD Fat-Sat WI of the right hip. Multiple tiny intra-articular bodies of...
. Multiple tiny intra-articular bodies of the same size. References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
Fig. 33:
Axial T1 WI of the right hip (arthro-MRI). Multiple tiny intra-articular bodies...
. Synovitis with some intra-articular bodies of different sizes. References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
Fig. 34:
Coronal PD WI of the left hip (arthro-MRI). Synovitis with some intra-articular...
. Synovitis with some intra-articular bodies of different sizes. References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
Fig. 35:
Sagital PD Fat-Sat WI of the left hip (arthro-MRI). Synovitis with some...
. References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
Fig. 36:
CR of the pelvis. Non-calcifying intra-articular bodies of the left hip (normal...

Fig. 37:
Coronal DP Fat-Sat WI of the right hip. Synovitis and focal single erosion of...

Fig. 38:
Coronal DP WI of the right hip. Synovitis and focal single erosion of the...
. Acetabular osteolytic lesion with discrete calcifications. References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
Fig. 39:
CT of the left hip (axial plane). Acetabular osteolytic lesion with discrete...
. Acetabular osteolytic lesion with discrete calcifications. References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
Fig. 40:
CT of the left hip (coronal plane). Acetabular osteolytic lesion with discrete...

Fig. 41:
CR of the left hip. Acetabular osteolytic lesion.

Fig. 42:
CR of the right hip. Femoral focal dense lesion on the inner facet of the...
. Femoral focal dense lesion on the inner cortex of the femoral neck (a nidus is seen). References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
Fig. 43:
CT of the right hip (coronal reformat). Femoral focal dense lesion on the inner...

Fig. 44:
CR of the left hip. Pathological fracture of the left hip due to metastatic...

Fig. 45:
Axial PD Fat-Sat WI of the left hip. Pathological fracture of the left hip due...

Fig. 46:
Coronal PD WI of the left hip. Pathological fracture of the left hip due to...

Fig. 47:
Coronal of the right hip. Pathological fracture of the right hip due to...
. References: Hospital da Luz - MSK Imaging Unit - Lisbon/PT")
Fig. 48:
Axial T1 WI of the pelvis. Right juxta-trochanteric mass with low-signal on T1...

Fig. 49:
Coronal T1 WI of the pelvis. Mass in the right inguinal area with low signal in...

Fig. 50:
Sagital PD Fat-Sat WI of the pelvis. Mass in the right inguinal area with high...