Imaging modalities including Intravenous urography (IVU) and Computed tomography (CT) technique,
sonography and Magnetic resonance imaging (MRI) are used in imaging of renal infections(1)
CT TECHNIQUE
- Non-contrast scan
- Nephrographic phase at 50-90 sec
- Excretory phase at 2 min if there is distal urinary tract obstruction (2)
ROLE OF MRI
- Apart from routine imaging sequences diffusion-weighted imaging has been applied as a problem solving tool to differentiate between hydronephrosis and pyonephrosis(Figure 1) and between focal pyelonephritis and renal cell carcinoma
- Pregnant patients
- Contraindication for iodinated contrast eg transplant patients
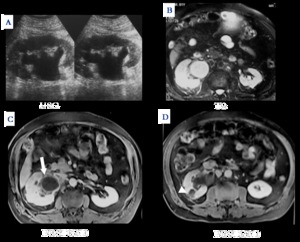
Fig. 1: PYELONEPHRITIS WITH PYONEPHROSIS:MR and USG imaging of a 42 year old male with right hydronephrosis and peripheral
enhancement of dilated PCS (arrow C) suggestive of pyonephrosis and heterogeneously enhancing focal lesion in right kidney (arrow D)
suggestive of focal pyelonephritis
References: Department of Radiology, All India Institute of Medical Sciences, New Delhi,2012
TABLE 1: SPECTRUM OF RENAL INECTIONS
|
ACUTE
|
CHRONIC
|
OTHERS
|
|
ACUTE PYELONEPHRITIS
|
CHRONIC PYELONEPHRITIS
|
TUBERCULOSIS
|
|
FOCAL NEPHRITIS
|
XANTHOGRANULOMATOUS PYELONEPHRITIS
|
FUNGAL
|
|
ABSCESS
|
MALAKOPLAKIA
|
|
|
EMPHSEMATOUS PYELONEPHRITIS
|
EOSINOPHILIC CYSTITIS
|
|
|
PAPILLARY NECROSIS
|
|
|
|
PYONEPHROSIS
|
|
|
ACUTE PYELONEPHRITIS
- Striated nephrogram ; an appearance described for acute pyelonephritis shows discrete rays of alternating hypoattenuation and hyperattenuation from the papilla to the cortex along the direction of the excretory tubules (Figure 2) .
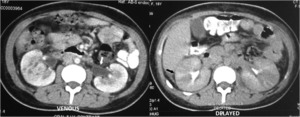
Fig. 2: ACUTE PYELONEPHRITIS:STRIATED NEPHROGRAM
Venous phase shows heterogeneous enhancement with pelvic wall thickening(arrow). Delayed phase shows alternating discrete rays of hyper and hypoattenuation suggesting striated nephrogram (black arrow)
References: Department of Radiology, All India Institute of Medical Sciences, New Delhi,2012
- This is ascribed to the decreased flow of contrast due to stasis and eventual hyperconcentration in the infected tubules
Different faces of pyelonephritis
- Wedge shaped zones of decreased attenuation
- Focal form as a hypodense mass (Figure 3a,b)
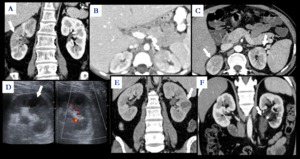
Fig. 3: DIFFERENT FACES OF ACUTE PYELONEPHRITIS : Focal wedge shaped hypodensity with surrounding fat stranding as in Right kidney in figure a and in left kidney in Figure b; or as smaller peripheral wedge shaped hypodensities as in Figure c.Figures d and e are showing focal hypodense well defined area in left kidney from a patient with acute pyelonephritis evolving into abscess.Figure f shows thickening and enhancement along left ureter and a pelvic calculus suggestive of Pyelitis
References: Department of Radiology, All India Institute of Medical Sciences, New Delhi
- Diffuse form- global enlargement,
poor enhancement of renal parenchyma,
absent excretion of contrast and streakiness of fat (Figure 2)
- Hemorrhagic bacterial nephritis which is relatively uncommon shows hyperattenuating areas representing parenchymal bleeding on non-contrast scan
*PEARLS
Differentials of striated nephrogram
- Not specific
- Also seen in renal vein thrombosis,
ureteric obstruction and contusion(3)
RENAL AND PERINEPHRIC ABSCESS
- Develop as a complication of focal pyelonephritis or hematogenous infection.
- Early abscess appears as poorly marginated non-enhancing area of decreased attenuation(Figure 4a,b).
- Mature abscess shows a sharply marginated complex cystic mass with necrosis and a peripheral enhancing rim (Figure 4c,d)
- USG may show internal echoes,
septations and loculations
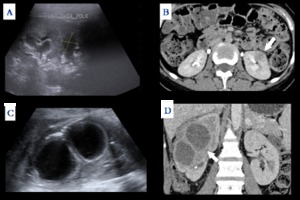
Fig. 4: Early abscess - Figure A USG shows focal hypoechoic lesion with few internal echoes corresponding to CT in Figure B
Mature abscess- Figure C USG shows complex cystic mass with thick wall corresponding to CT in Figure D
References: Department of Radiology, All India Institute of Medical Sciences, New Delhi,2012
- Diffusion weighted (DW)-MRI can readily pick up abscesses which show marked restriction of diffusion(Figure 5)
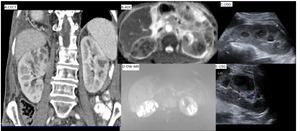
Fig. 5: PYOGENIC ABSCESSES: CECT of a middle aged diabetic male revealed multiple peripherally enhancing lesions with crenated margins in bilateral kidneys . The lesions were bright on DW-MRI and dark on ADC map suggestive of restricted diffusion. Sampling revealed this patient to have pyogenic abscesses. The lesions resolved after antibiotic therapy.
References: Department of Radiology, All India Institute of Medical Sciences, New Delhi,2012
- In transplant patientsMR has an important role to play as iodinated contrast may be contraindicated due to abnormal renal function (Figure 6)
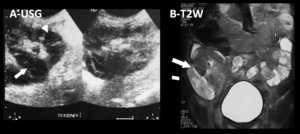
Fig. 6: PYELONEPHRITIS WITH TRANSPLANT ABSCESS
USG of a 25 year old transplant patient shows multiple hypoechoic lesions within the cortex(arrowhead A) with one large lesion laterally(arrow A). MR shows multiple hyperintensities in the renal cortex and a large well defined abscess laterally(arrow B).
References: Department of Radiology, All India Institute of Medical Sciences, New Delhi,2012
PYONEPHROSIS
- Infection in an obstructed collecting system; the cause of obstruction may be a calculus,
stricture,
tumour or congenital anomaly
- USG shows dilated PCS with debris and fluid-fluid levels within (Figure 7)(1)

Fig. 7: PYONEPHROSIS-USG shows typical dilated calyces with echogenic debris within
References: Department of Radiology, All India Institute of Medical Sciences, New Delhi,2012
- On CT dilated pelvicalyceal system with hyperdense urine and contrast layering with associated parenchymal or perinephric inflammatory changes and thickening of pelvic wall suggest infection (Figure 8a,b).
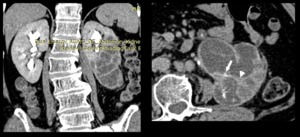
Fig. 8: PYONEPHROSIS IN DUPLEX MOEITY
Delayed phase CECT: Left kidney shows hydronephrosis with poor contrast excretion in the middle and lower calyces (Coronal MPR) suggestive of duplex kidney with obstructed lower moeity. Walls of left PCS show thickening and inflammation(arrowhead) and crescentic enhancement (arrow) suggesting pyonephrosis
References: Department of Radiology, All India Institute of Medical Sciences, New Delhi,2012
- Diffusion weighted imaging may have an additional role in distinguishing hydronephrosis from pyonephrosis (Figure 9).
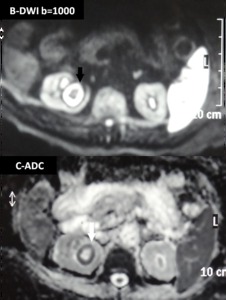
Fig. 9: PYONEPHROSIS:
DWI and ADC maps show restricted diffusion within the dilated pelvicalyceal system suggestive of pyonephrosis
References: Department of Radiology, All India Institute of Medical Sciences, New Delhi,2012
- Treatment is immediate Percutaneous nephrostomy
XANTHOGRANULOMATOUS PYELONEPHRITIS
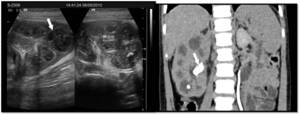
Fig. 10: XANTHOGRANULOMATOUS PYELONEPHRITIS: USG shows enlarged kidney with parenchyma replaced with multiple hypoechoic masses comprising inflammatory exudates. CT shows multiple low-attenuation rounded masses, corresponding to either dilated calyces or focal areas of parenchymal destruction and a central staghorn calculus (arrow)
References: Department of Radiology, All India Institute of Medical Sciences, New Delhi,2012
- Chronic granulomatous process affecting middle aged females and children.
- Recurrent E coli and Proteus mirabilis infection
- Ninety percent have a stagnorn calculus.
- Pathologically there is replacement of renal parenchyma with foamy macrophages
- USG- Multiple hypoechoic masses with a central calculus
- CT-Low attenuation rounded masses which represent dilated calyces and abscess cavities filled with inflammatory exudates (Figure 10a,b).
- Diffuse(80%) or focal(15%) form which are treated by nephrectomy or partial nephrectomy respectively.
*PEARLS
|
Atypical features:
- Absence of calculi 10%
- Focal instead of diffuse 10%
- Atrophy instead of enlargement
|
|
Typical features
- Non-functioning enlarged kidney
- Central calculus
- Expansion of calices with hypodense material
- Inflammatory changes in the perinephric fat
|
|
|
TABLE 2
EMPHYSEMATOUS PYELONEPHRITIS
- Life threatening necrotising infection with gas formation
- Associated with Diabetes Mellitus or immunocompromised status
- Presence of gas is attributed to fermentation due to bacteria in the presence of high glucose levels (4)
- Two forms depending on severity and prognosis (Table 3)
Table 3: Emphysematous pyelonephritis
|
|
TYPE 1 -33%
|
TYPE 2 -66%
|
|
Parencymal destruction
|
Severe –streaky gas radiating from medulla to cortex with crescent of subcapsular gas
|
Lesser
|
|
Fluid collecion
|
None as the reduced immune response limits pus collection
|
Renal or perirenal fluid collection is characteristic
|
|
Mortality
|
80%
|
20%
|
|
Treatment
|
Nephrectomy
|
Aggressive medical treatment with percutaneous drainage
|
- USG shows non-dependent echoes within the parenchyma and collecting system with dirty shadowing (Not sensitive to small amounts of gas)
- CT is done to determine severity and extent of disease and to detect parenchymal destruction,
fluid collections and abscess formation (Figure 11)
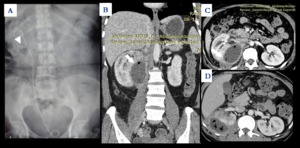
Fig. 11: EMPHYSEMATOUS PYELONEPHRITIS:
Figure A -52 year diabetic female; radiograph of abdomen shows speck of air(arrowhead) overlying lower pole of right kidney with a DJ stent in situ. Figure B&C CECT abdomen shows a well defined collection causing compression on right kidney with air foci within and peripheral fat stranding suggestive of Type B emphysematous pyelonephritis
Figure D 47 year male shows similar yet more extensive gas collection within perirenal fluid collection with surrounding inflammatory changes
References: Department of Radiology, All India Institute of Medical Sciences, New Delhi,2012
Emphysematous cystitis
- Air fluid level in the bladder lumen or linear streaks of air in the bladder wall (Figure 12).

Fig. 12: EMPHYSEMATOUS CYSTITIS:
CECT of a diabetic lady who clinically presented as urinary infection shows bladder wall thickening and air within the bladder.
References: Department of Radiology, All India Institute of Medical Sciences, New Delhi,2012
Emphysematous pyelitis
- Accompanies obstruction of PCS by a calculus,
neoplasm or stricture
- 50% are diabetics (4)
- CT shows gas within the dilated PCS and urinary bladder(Figure 13)
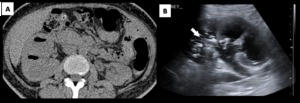
Fig. 13: EMPHYSEMATOUS PYELITIS:42 year old diabetic lady. NCCT (Figure a) shows gas within dilated PCS. USG(Figure b) shows echoes within the PCS with dirty shadowing
References: Department of Radiology, All India Institute of Medical Sciences, New Delhi,2012
*PEARLS
- Before making a diagnosis of emphysematous cystitis history of instrumentation must be ruled out
- The distinction between emphysematous pyelitis and pyelonephritis is important; as the former is a less aggressive infection and does not require nephrectomy
- In pyelitis air is limited to PCS while pyelonephritis it enters the parenchyma
CHRONIC PYELONEPHRITIS
- Etiology - reflux of infected urine in childhood,
recurrent infections or as a result of a remote single infection(5)
- Imaging shows focal polar scars with underlying calyceal distortion with global atrophy and hypertrophy of residual tissue (Figure 14)
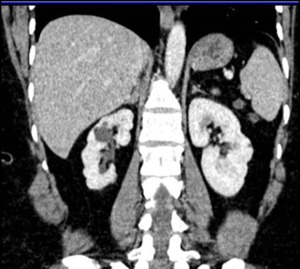
Fig. 14: CHRONIC PYELONEPHRITIS: CECT shows asymmetrically atrophic right kidney with scars overlying the dilated calyces, typical of chronic pyelonephritis
References: Department of Radiology, All India Institute of Medical Sciences, New Delhi,2012
*PEARLS
- Lobar infarcts can be differentiated from chronic pyelonephritis by the lack of calyceal involvement
- Fetal lobulations are differentiated by depressions lying between calyces rather than overylying calyces.
GENITOURINARY (GU) TUBERCULOSIS
|
IVP FINDINGS
- Earliest -caliectasis with irregular contour (arrow Figure 15)
- Phantom calyx
- Cavity communicating with deformed calyx (Figure 16)
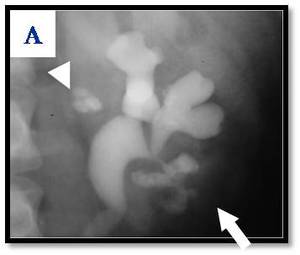 Fig. 15: Early TB: infundibular stenosis (arrowhead) and irregular caliectasis with feathery contour (arrow)
References: Department of Radiology, All India Institute of Medical Sciences, New Delhi,2012
 Fig. 16: Genitourinary-TB: Delayed CT image showing a cavity in lower pole of right kidney communicating with calyx-characteristic of Genitourinary TB
References: Department of Radiology, All India Institute of Medical Sciences, New Delhi,2012 RENAL INVOLVEMENT
occurs in 3 forms
A- Unifocal or multifocal mass lesions
B-Scarred papillae, dilated calyces,
hiked up pelvis
C-Autonephrectomy-poorly excreting
Caseocavernous type-enlarged sac filled with caseous material
Calcified shrunken kidney Figure 17 ,18 (6)
|
 Fig. 17: PUTTY KIDNEY:Radiograph showing end stage renal tuberculosis-entirely calcified right kidney
References: Department of Radiology, All India Institute of Medical Sciences, New Delhi,2012
 Fig. 18: NCCT showing right putty kidney
References: Department of Radiology, All India Institute of Medical Sciences, New Delhi,2012
URETER
Stricture terminal segment
- Beaded appearance
- Pipe stem ureter-rigid shortened (Figure 19)
- Narrowed lumen
 Fig. 19: PIPESTEM URETER:IVP image of a patient with Genitourinary TB shows dilated left ureter with intermittent irregular narrowing
References: Department of Radiology, All India Institute of Medical Sciences, New Delhi,2012 |
Tabe 4
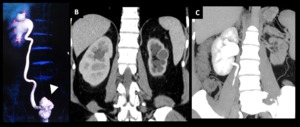
Fig. 20: Genitourinary-TB: THIMBLE bladder (Figure A arrowhead),hiked up right renal pelvis and hydroureteronephrosis. Left kidney is shrunken, contracted with cortical thinning(Figure B)and non-excretion on delayed image (Figure C)
References: Department of Radiology, All India Institute of Medical Sciences, New Delhi,2012
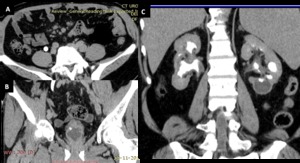
Fig. 21: GU-TB:Bilateral hydronephrosis with left lower pole,CT correlate of phantom calyx(Figure C arrow), thimble bladder with multiple diverticulae (Figure B).This patient also had mesentric lymhadenopathy (Figure A arrowhead)
References: Department of Radiology, All India Institute of Medical Sciences, New Delhi,2012
PARASITIC INFECTION
Schistosomiasis
- ACUTE PHASE: nodular bladder wall thickening
- CHRONIC PHASE: contracted,
fibrotic,
thick-walled bladder with typical curvilinear calcifications
- Premalignant condition
Hydatid disease
- Most commonly involves the liver; renal hydatids comprise 5% patients
- Renal hydatid - unilocular or multilocular cystic lesion with or without peripheral calcification (Figure 22 )(7)
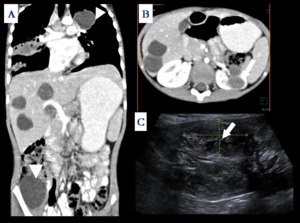
Fig. 22: DISSEMINATED HYDATIDOSIS: Figure A shows unilocular cysts in mediastinum(arrowhead), lung, liver and right iliacus (arrowhead). Figure B shows additional cysts in left kidney. USG (Figure C) shows multiple unilocular cystic lesions with membrane like structures within (arrow)
References: Department of Radiology, All India Institute of Medical Sciences, New Delhi,2012
FUNGAL INFECTION
- Severe life threatening infection
- RISK FACTORS : diabetes mellitus,
haematological malignancy,
HIV and other immunocompromised conditions
- COMMON ORGANISMS :candida and aspergillus
- Acquired by hematogenous or ascending route.
- IMAGING FINDINGS
- Renal microabscesses- hypoattenuating lesions with a striated nephrogram (Figure 23a)
- Fungal ball –due to conglomeration of fungal hyphae and inflammatory cells which appears as an irregular filling defect in the collecting system
- Mucor-rare organism which has a tendency to invade vessels and cause infarction
- High mortality
- Requires combined surgical and medical manangement to improve outcome (figure 23 b,c,d,e)(8)
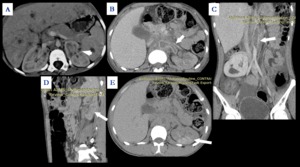
Fig. 23: FUNGAL INFECTION:
CECT shows liver, spleen and bilateral kidneys studded with small microabscesses in a 10 year old leukemia patient proven to have Aspergillus infection on sampling.B-nephrographic C,D,E-delayed phase of another 26 year old acute aplastic anemia patient. CECT shows poorly enhancing, non-excreting left kidney with perinephric inflammation. There is a thrombus in left renal artery and aorta(arrow Figure C). On delayed image (Figure E) striated nephrogram in left kidney is seen. FNAC from the perirenal soft tissue revealed fungal hyphae and diagnosis of angioinvasive fungal infection (mucor) was made and he was started on Amphotericin B. However patient expired two days later.
References: Department of Radiology, All India Institute of Medical Sciences, New Delhi,2012
Pneumocystic carini infection
- HIV patients
- Diffuse punctuate calcifications in kidneys and organs of the reticuloendothelial system (9)
EOSINOPHILIC CYSTITIS
- Rare chronic inflammatory disease of urinary bladder due to eosinophil infiltration into bladder wall leading to fibrosis and muscle necrosis
- Clinically presents as hematuria,
frequency and irritative symptoms in a middle aged individual (10)
- Imaging: Diffuse bladder wall thickening often more than 10 mm with characteristic preservation of the mucosal line and enhancement on delayed images (Figure 24a,b)(10)
*PEARLS
- Differential: neoplastic etiology is a close differential therefore biopsy is essential
- Associated diffuse or segmental bowel wall thickening and hepatic nodules
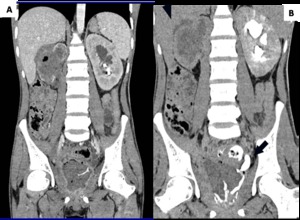
Fig. 24: EOSINOPHILIC CYSTITIS: nephrographic and delayed phases of a 25 year old man who presented with hematuria and worsening irritative symptoms over past one year. Clinical suspicion was that of a bladder malignancy. CECT shows diffuse mass like bladder wall thickening and irregularity with air specks in the wall, mass like soft tissue replacing entire kidney with perinephric spread. On the delayed phase (Figure B) there is opacification of rectum suggestive of a fistulous communication. Note is made of striated nephrogram in left kidney suggesting ongoing acute inflammatory process. Biopsy revealed eosinophilic infiltration and fibrosis within the bladder wall with no evidence of malignancy suggestive of eosinophilic cystitis.
References: Department of Radiology, All India Institute of Medical Sciences, New Delhi,2012

 suggestive of pyonephrosis and heterogeneously enhancing focal lesion in right kidney (arrow D)
suggestive of focal pyelonephritis References: Department of Radiology, All India Institute of Medical Sciences, New Delhi,2012")
. Delayed phase shows alternating discrete rays of hyper and hypoattenuation suggesting striated nephrogram (black arrow) References: Department of Radiology, All India Institute of Medical Sciences, New Delhi,2012")



 with one large lesion laterally(arrow A). MR shows multiple hyperintensities in the renal cortex and a large well defined abscess laterally(arrow B). References: Department of Radiology, All India Institute of Medical Sciences, New Delhi,2012")

 suggestive of duplex kidney with obstructed lower moeity. Walls of left PCS show thickening and inflammation(arrowhead) and crescentic enhancement (arrow) suggesting pyonephrosis References: Department of Radiology, All India Institute of Medical Sciences, New Delhi,2012")

 References: Department of Radiology, All India Institute of Medical Sciences, New Delhi,2012")
 overlying lower pole of right kidney with a DJ stent in situ. Figure B&C CECT abdomen shows a well defined collection causing compression on right kidney with air foci within and peripheral fat stranding suggestive of Type B emphysematous pyelonephritis
Figure D 47 year male shows similar yet more extensive gas collection within perirenal fluid collection with surrounding inflammatory changes References: Department of Radiology, All India Institute of Medical Sciences, New Delhi,2012")

 shows gas within dilated PCS. USG(Figure b) shows echoes within the PCS with dirty shadowing References: Department of Radiology, All India Institute of Medical Sciences, New Delhi,2012")

 and irregular caliectasis with feathery contour (arrow) References: Department of Radiology, All India Institute of Medical Sciences, New Delhi,2012")




,hiked up right renal pelvis and hydroureteronephrosis. Left kidney is shrunken, contracted with cortical thinning(Figure B)and non-excretion on delayed image (Figure C) References: Department of Radiology, All India Institute of Medical Sciences, New Delhi,2012")
, thimble bladder with multiple diverticulae (Figure B).This patient also had mesentric lymhadenopathy (Figure A arrowhead) References: Department of Radiology, All India Institute of Medical Sciences, New Delhi,2012")
, lung, liver and right iliacus (arrowhead). Figure B shows additional cysts in left kidney. USG (Figure C) shows multiple unilocular cystic lesions with membrane like structures within (arrow) References: Department of Radiology, All India Institute of Medical Sciences, New Delhi,2012")
. On delayed image (Figure E) striated nephrogram in left kidney is seen. FNAC from the perirenal soft tissue revealed fungal hyphae and diagnosis of angioinvasive fungal infection (mucor) was made and he was started on Amphotericin B. However patient expired two days later. References: Department of Radiology, All India Institute of Medical Sciences, New Delhi,2012")
 there is opacification of rectum suggestive of a fistulous communication. Note is made of striated nephrogram in left kidney suggesting ongoing acute inflammatory process. Biopsy revealed eosinophilic infiltration and fibrosis within the bladder wall with no evidence of malignancy suggestive of eosinophilic cystitis. References: Department of Radiology, All India Institute of Medical Sciences, New Delhi,2012")