ECR 2013 / C-2165
Unexpected Hosts: Imaging Parasitic Diseases
Congress:
ECR 2013
Poster Number:
C-2165
Type:
Educational Exhibit
Keywords:
Abdomen, CNS, Ultrasound, CT, MR, Diagnostic procedure, Infection, Parasites
Authors:
P. Hernández , P. Rodriguez Carnero, S. Martin Garre; Madrid/ES
DOI:
10.1594/ecr2013/C-2165

Table 1

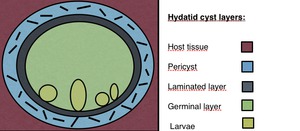
Fig. 1:
Hydatid cyst structure. Pericyst: it is the outer layer and is fundamentally...
 in a 75 year old patient found incidentally.")
Fig. 2:
Anteroposterior abdomen radiograph showing an hepatic calcified hydatid cyst...

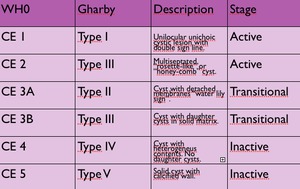
Table 2:
WHO and Gharby comparative ultrasound classification on echinococcal cysts.

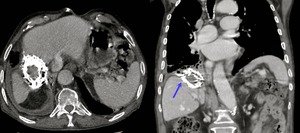
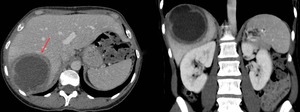
Fig. 3:
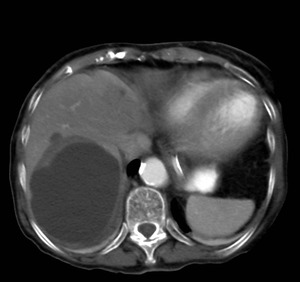
Axial and coronal CT views showing a calcified hepatic hydatid cyst with...
.")
Fig. 4:
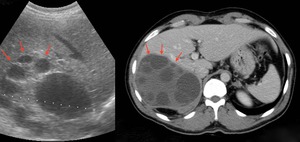
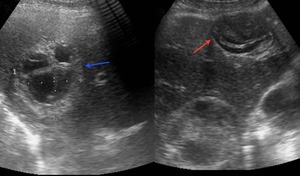
Sagital sonogram and axial enhanced scan showing a multivesicular hydatid cyst....
. The other one shows a different appearance, an hydatid cyst with daughter vesicles. Note that the daughter cysts occupy almost the entire volume of the mother cyst (rosette sign).")
Fig. 5:
Sagital sonogram showing two hydatid cysts. Note that one of them contains...

Fig. 6:
Axial enhanced CT scan showing an unilocular hydatid hepatic cyst.

Fig. 7:
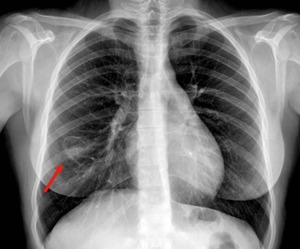
Posteroanterior chest radiograph showing a cavitary lesion in the right...
.")
Fig. 8:
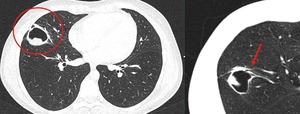
Axial high resolution CT showing the hydatid cyst with solid content. Axial...
.")
Fig. 9:
Multiple peritoneal hydatid cysts secondary to seeding of a ruptured hepatic...
.")
Fig. 10:
Renal hydatid cyst with heterogeneus content on an axial enhanced CT scan. Note...

Fig. 11:
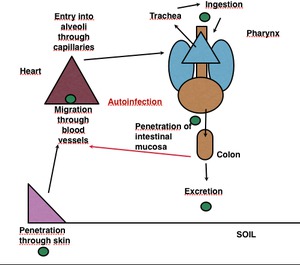
Life cycle of S. stercolaris in the human body.
.")
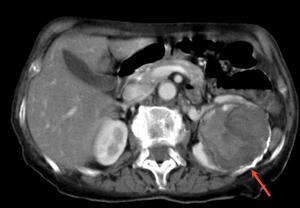
Fig. 12:
Axial abdominopelvic unhenanced scan of an inmunocompromised 45 year-old...

Fig. 13:
Axial chest unhenanced scan of an inmunocompromised 45 year-old patient...

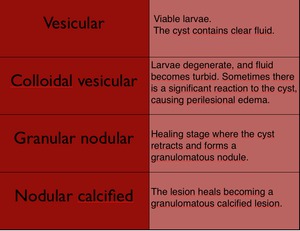
Table 3:
Developmental stages of Neurocysticercosis

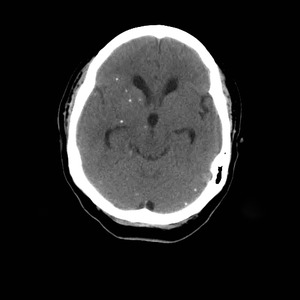
Fig. 14:
Axial non-enhanced CT of the brain show multiple, punctate, calcified nodules...

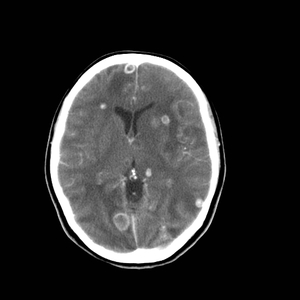
Fig. 15:
Axial enhanced CT of the brain showing multiple enhancing lesions surrounded by...
 hyperintense to CSF with no edema and no rim enhancement.")
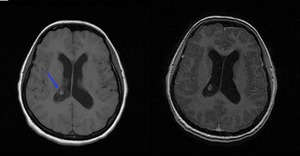
Fig. 16:
Subarachnoid vesicular neurocysticercosis. Axial T1-WI and axial T1-WI...
 and one of them surrounded by edema (blue arrow) in a neurocysticercosis at a colloidal vesicular stage.")
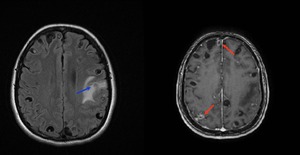
Fig. 17:
Axial fluid-attenuated inversion recovery and axial T1-WI gadolinium enhanced...
, mild mass effect and surrounding edema in the right hemisphere of cerebellum.")
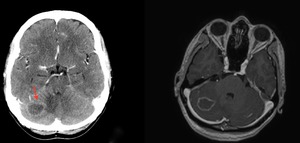
Fig. 18:
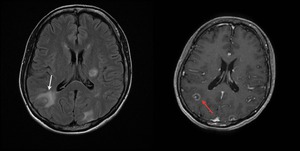
Intracranial toxoplasmosis in a 45 year-old patient with AIDS. Axial enhanced...
, and ring enhancement (red arrow).")
Fig. 19:
Axial fluid-attenuated inversion recovery and T1-WI gadolinium enhanced MR...

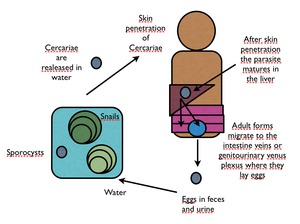
Fig. 20:
Schistosoma species life cycle.
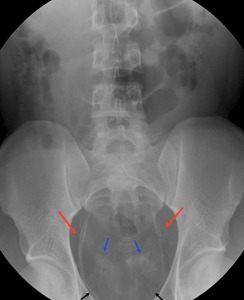
, calcified vas deferens (blue arrows) and bladder (black arrows). Case courtesy J.Barrera/ES")
Fig. 21:
Anteroposterior abdomen radiograph showing calcification of the pelvic segment...

Fig. 22:
Anteroposterior pelvis radiograph showing a totally calcified bladder in a...

Fig. 23:
Axial sonogram showing rounded, well-defined cystic hypoechoic lesion with...
.")
Fig. 24:
Axial and coronal enhanced CT scan images showing a large cystic mass in the...

Fig. 25:
Posteroanterior and lateral knee radiograph showing multiple calcified Guinea...

Fig. 26:
A barium enema of a 42 year-old Bolivian patient showing megacolon,...
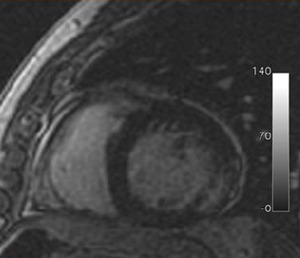
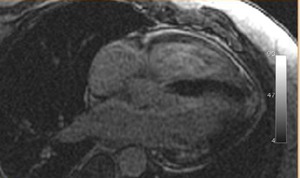
, indicating myocardial fibrosis or necrosis.
Case courtesy B.Cabeza and A.Bustos/ES")
Fig. 27:
Cardiac chronic Chagas disease. South American male diagnosed of T. cruzi...

Fig. 28:
Cardiac chronic Chagas disease. South American male diagnosed of T. cruzi...

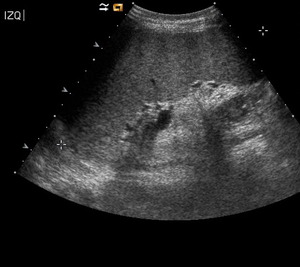
Fig. 29:
Axial sonogram showing esplenomegaly in a 52 year-old patient presenting with...

Fig. 30:
Axial enhanced CT scan showing hepatoesplenomegaly in a patient with visceral...