Imaging Findings or Procedure Details
Analysis included history; findings at physical examination,
mammography,
ultrasonography,
MRI and histologic type of inflammatory carcinoma.
Mammography Findings
Mammography in two standard planes of imaging (craniocaudal and mediolateral oblique) was performed,
sometimes with additional views.
The most common mammographic findings are diffuse or focal skin thickening (skin of the involved breast is thicker than that of the contralateral breast),
trabecular prominence and diffusely increased breast density compatible with edema.
Other findings can be presente,
such as nipple retraction,
presence of a mass,
asymmetric focal density (asymmetry of tissue density with a similar shape seen on two views but completely lacking borders and the conspicuity of a true mass),
microcalcifications,
and axillary lymphadenopathy.
Most commonly the microcalcifications are pleomorphic or linear and branching,
suggestive of malignancy .
But they can be diffuse,
scattered,round,
or punctate meant that they are considered benign or probably benign.
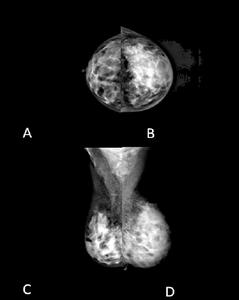
Fig. 1: Mammograms are of a 45 -year-old woman with clinically evident IC.
A,B Craniocaudal and C,D mediolateral oblique views of both breasts are shown. A central mass is present. Left breast was enlarged, the right breast is normal.
Diffusely increased opacity, stromal coarsening, and skin thickening are seen on the left when compared with the contralateral breast.
US Findings
All patients underwent both axillary and breast US,
which was performed either to detect or to evaluate solid masses or axillary lymphadenopathy.
When a mass was present,
the location,
size,
contour,
and acoustic features were evaluated.
US findings : skin thickening ( skin of the involved breast was thicker than that of the contralateral breast),
skin invasion (interruption deep echogenic line of the skin,
the dermis,
or the subcutaneous fat interface),
dilated lymphatic channels (branching anechoic tubular structures in the subcutaneous fatty tissues),
pectoral muscle invasion (the mass was in contact with the pectoral muscle,
and the tissue planes in between were obliterated),
multifocality (the mass are within the same quadrant),
multicentricity (the mass are in different quadrants),
increased vascularity on color Doppler.
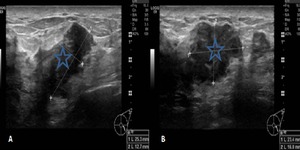
Fig. 2: Images obtained in a 43-year-old woman with a mass measuring 3cm in longest diameter in the upper outer quadrant of the left breast, peau d’orange, and nipple retraction.
A,B Transverse US scans show marked skin thickening. Hypoechoic masses are also seen with posterior acoustic shadowing. The mass limits was hard to demonstrate because the breast was thick owing to parenchymal edema.
Axillary lymphadenopathy are identified on the basis of the following criteria: nodular cortical appearance and cortical thickness larger than 3mm,
replacement of fatty hilum and round shape.
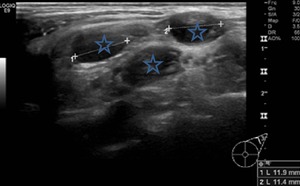
Fig. 3: Image obtained in a 45-year-old woman with a palpable mass in the upper quadrant of the left breast and breast erythema.
Round axillary, supra-clavicular and cervical nodes with increased density and loss of lucent fatty hilum are consistent with lymphadenopathy with metastatic disease.
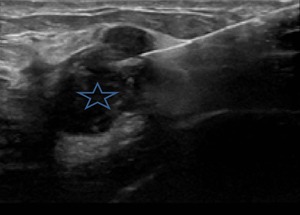
Fig. 4: Ultrasound-guided core needle biopsy obtained in a 45-year-old woman with a mass 3cm in longest diameter in the upper outer quadrant of the left breast. Histologic subtype: invasive ductal carcinoma.
MR Findings
The breast should be imaged at axial,
coronal or sagittal planes.
Core pulse sequences when evaluating the breast for cancer include a three-plane localizer,
T1WIs,
T2WIs,
and two- or three-dimensional fat-suppressed gradient echo series performed before contrast administration,
immediately after,
and delayed.
The number of postcontrast series can vary,
but at least three are needed to perform kinetic enhancement curves.
The T1WIs allow clear differentiation of adipose tissue from glandular tissue.
T2W fat-suppressed images allow identification of fluid-filled structures such as cysts.
Dynamic images obtained prior to and after IV gadolinium enhancement help to identify potential malignancies based on morphology and enhancement kinetics.
The intravenous gadolinium DTPA dose ranges from 0.1 to 0.2 mmol/kg body weight.
In posterior breast masses,
MRI can identify muscle invasion (muscle enhancement on MR images) with accuracy.
Fat suppression can be accomplished before gadolinium administration using chemical selective fat saturation or water-only excitation techniques.
After IV contrast administration,
passive fat suppression can be accomplished with post processing image subtraction,
but patient movement between precontrast and postcontrast enhanced images can degrade the images because of misregistration.
Kinetic curves can be performed on enhancing lesions.
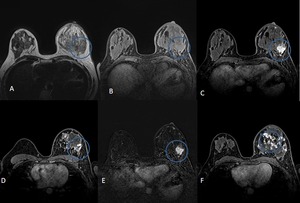
Fig. 5: Axial MR images obtained in a 43-year-old woman with a mass in the upper outer quadrant of the left breast, peau d’orange, and nipple retraction.
(A) T2WIs (B) T1WIs Precontrast (C;D), early postcontrast, and late postcontrast (E,F) enhanced fat-suppressed T1W fast spoiled gradient-echo MR images of the left breast show multifocal spiculated enhancing mass at left breast. The mass demonstrates rapid initial mass enhancement without pectoral muscle involvement. Note the skin enhancement, pointing to edema and nflammatory alterations.
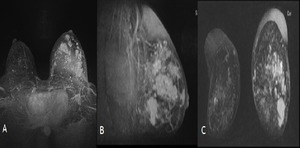
Fig. 6: Axial (A) sagittal (B) and coronal (C) MIP reformated images obtained in a 43-year-old woman with a mass in the upper outer quadrant of the left breast, peau d’orange, and nipple retraction.
Kinetic curves improve the specificity of breast MR.
These curves can be evaluated qualitatively according to the curve shape and classified as a persistent pattern of enhancement,
a plateau of enhancement,
or washout of signal intensity.
Most invasive carcinomas demonstrate rapid initial enhancement with a plateau or washout.
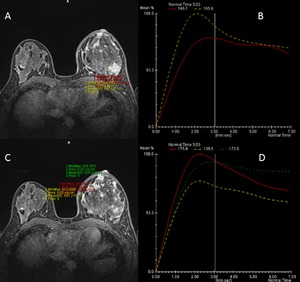
Fig. 7: Axial MR images obtained in a 43-year-old woman with a mass at upper outer quadrant of the left breast, which was enlarged with peau d’orange, and nipple retraction.
(A,B,C,D) Kinetic curves demonstrates rapid initial enhancement of multifocal mass with a plateau and washout pointing to carcinoma.
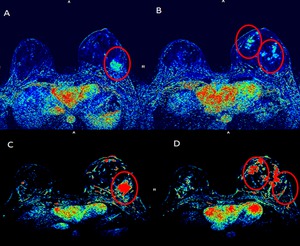
Fig. 8: Axial MR images obtained in a 45-year-old woman with a mass in the upper outer quadrant of the left breast, which was enlarged with peau d’orange, and nipple retraction.
(A,B,C,D) washout maps demonstrate multifocal mass with a plateau or washout pointing to carcinoma.





 sagittal (B) and coronal (C) MIP reformated images obtained in a 43-year-old woman with a mass in the upper outer quadrant of the left breast, peau d’orange, and nipple retraction.")
 Kinetic curves demonstrates rapid initial enhancement of multifocal mass with a plateau and washout pointing to carcinoma.")
 washout maps demonstrate multifocal mass with a plateau or washout pointing to carcinoma.")
 T2WIs (B) T1WIs Precontrast (C;D), early postcontrast, and late postcontrast (E,F) enhanced fat-suppressed T1W fast spoiled gradient-echo MR images of the left breast show multifocal spiculated enhancing mass at left breast. The mass demonstrates rapid initial mass enhancement without pectoral muscle involvement. Note the skin enhancement, pointing to edema and nflammatory alterations.")