ECR 2013 / C-2454
THROUGH THE EYES OF THE TRANSPLANT SURGEON - Multidetector CT angiography in evaluating renal vasculature- Preoperative implications
Congress:
ECR 2013
Poster Number:
C-2454
Type:
Educational Exhibit
Keywords:
Transplantation, Congenital, Aneurysms, Computer Applications-Detection, diagnosis, Computer Applications-3D, CT-Angiography, Kidney
Authors:
Z. Ahmad1, C. J. Das2, S. Kumar1, K. Rangarajan1, S. Sharma3, A. K. Gupta1; 1New Delhi/IN, 2Dehli/IN, 3NEW DELHI, DELHI/IN
DOI:
10.1594/ecr2013/C-2454

Fig. 1:
Renal vascular anatomy

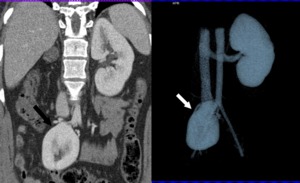
Fig. 2:
AGENESIS: Coronal CECT showing left renal agenesis

Fig. 3:
HORSESHOE KIDNEY: VRT showing medially oriented lower renal poles joining...

Fig. 4:
ADULT POLYCYSTIC KIDNEY DISEASE

Fig. 5:
Coronal MPR and VRT images show a malrotated ectopic right kidney. This serves...

Fig. 6:
MULTIPLE ARTERIES: Coronal MIP image showing three hilar arteries supplying the...

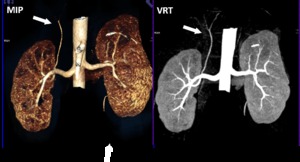
Fig. 7:
ACCESSORY HILAR ARTERY :MIP and VRT images showing bilateral accessory hilar...

Fig. 8:
POLAR ARTERY: Coronal MIP showing right superior polar artery with a...
.It normally arises from aorta. References: Department of Radiology, All India Institute of Medical Sciences, New Delhi,2012")
Fig. 9:
VARIANT INFERIOR PHRENIC ARTERY: VRT AND MIP images showing right inferior...

Fig. 10:
PREHILAR BIFURCATION:
x=distance of right renal artery from right IVC margin
...

Fig. 11:
PREHILAR POLAR ARTERY: MIP and VRT images showing right accessory polar artery...

Fig. 12:
MIP image showing right accessory hilar artery and left perhilar bifurcation
causes a "string of beads" appearance in mid and distal renal artery References: V Baliyan, Department of Radiology, AIIMS, New Delhi")
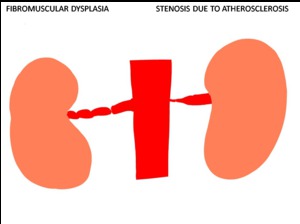
Fig. 13:
Renal artery stenosis due to atherosclerosis causes ostial narrowing while...

Fig. 14:
FIBROMUSCULAR DYSPLASIA: MIP image showing "string of beads" appearance in mid...

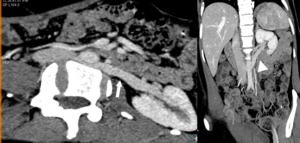
Fig. 15:
RENAL ARTERY STENOSIS: MIP and VRT images show ostial narrowing in right renal...

Fig. 16:
DOUBLE RENAL VEINS: MIP image shows two renal veins on right side

Fig. 17:
TRIPLE RENAL VEINS: MIP and VRT images showing three renal veins on the right...
 References: Department of Radiology, All India Institute of Medical Sciences, New Delhi,2012")
Fig. 18:
LARGE GONADAL VEIN: Gonadal vein more than 5mm is to be reported as seen in...
, circumaortic course(B) and retroaortic course(C) References: V Baliyan, Department of Radiology, AIIMS, New Delhi")
Fig. 19:
Diagram showing normal course of left renal vein anterior to aorta(A),...

Fig. 20:
CIRCUMAORTIC RENAL VEIN

Fig. 21:
RETROAORTIC RENAL VEIN: Oblique and Coronal MPRs show retroaortic and obliquely...

Fig. 22:
DOUBLE IVC: right IVC and left IVC shown by arrow and arrowhead respectively
 continuing upward from the right renal vein. Left IVC(arrowhead) is draining the lower limb and left renal vein References: Department of Radiology, All India Institute of Medical Sciences, New Delhi,2012")
Fig. 23:
MIP and VRT images showing right IVC(arrow) continuing upward from the right...

Fig. 24:
LATE SEGMENTAL CONFLUENCE: x=distance from right renal vein confluence to right...
 References: Department of Radiology, All India Institute of Medical Sciences, New Delhi,2012")
Fig. 25:
LATE SEGMENTAL CONFLUENCE: Curved MPR images show that left renal segemental...

Fig. 26:
PARTIAL DUPLICATION OF RIGHT URETER

Fig. 27:
SMALL RENAL CALCULUS: can be transplanted without calculus removal

Fig. 28:
MULTIPLE CALCULI: must be removed prior to transplantation

Fig. 29:
BOSNIAK TYPE 1 CYST: can be transplanted
: must be excised prior to transplantation References: Department of Radiology, All India Institute of Medical Sciences, New Delhi,2012")
Fig. 30:
ANGIOMYOLIPOMA (fat density lesion in right kidney): must be excised prior to...

Fig. 31:
ANGIOMYOLIPOMA: T1W image shows hyperintense lesion in rigt kidney...

Fig. 32:
RENAL ONCOCYTOMA: well defined lesion in the left kidney showing arterial...