ECR 2013 / C-2543
Septic arthritis of the pubic symphysis: Report of 5 cases and review of literature
Congress:
ECR 2013
Poster Number:
C-2543
Type:
Scientific Exhibit
Keywords:
Infection, Arthritides, Acute, Laboratory tests, Diagnostic procedure, Comparative studies, MR, CT-High Resolution, Conventional radiography, Pelvis, Musculoskeletal system, Musculoskeletal joint
Authors:
J. Quispe Bravo1, J. A. Narváez2, G. C. Rivera Sierra3, J. Hernández Gañán4, E. De Lama Salvador5, R. Mast2; 1L´Hospitalet de Llobregat (Barcelona) , ESP/ES, 2HOSPITALET DE LLOBREGAT/ES, 3L´Hospitalet de Llobregat (Barcelona) /ES, 4L' Hospitalet de Llobregat/ES, 5Barcelona/ES
DOI:
10.1594/ecr2013/C-2543

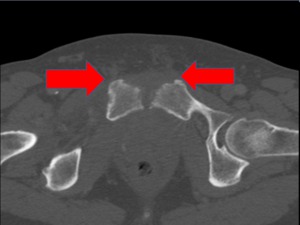
Fig. 1:
Fig 1 Case 1. Septic arthritis of the pubic symphysis. Image showing joint...

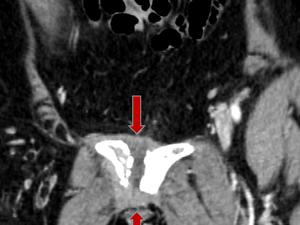
Fig. 2:
Case 1.- Contrast-enhanced coronal CT.Septic arthritis of the pubic symphysis....

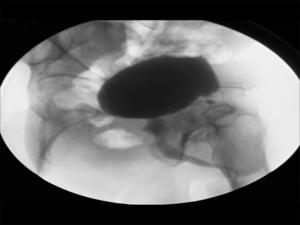
Fig. 4:
Fig 4 case 1.- Radiography of the pelvis, which shows pubic symphysis sclerosis...

Fig. 5:
Case 2. 64-year-old man. Contrast-enhanced axial pelvic CT reveals fluid in...

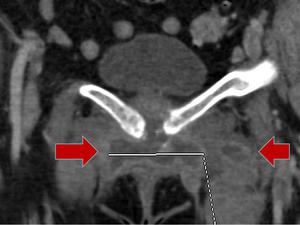
Fig. 3:
Fig 3. Case 1. Septic arthritis of the pubic symphysis. Volume rendering image.

Fig. 7:
Case 2 . 64-year-old man. Cortical destruction at the pubic symphysis. Axial TC

Fig. 8:
Case 2. Septic arthritis of the pubic symphysis in a 64-year-old. Plain A-P...

Fig. 14:
Case 3. 60-year-old female.
Signs of septic arthritis of the pubic symphysis,...

Fig. 13:
Case 3. Septic arthritis of the pubic symphysis caused by Staphylococcus aureus...

Fig. 6:
Case 2. Septic arthritis of the pubic symphysis in a 64-year-old man. Axial CT....

Fig. 12:
Case 3. Erosions with joint space widening
Contrast-enhanced coronal CT.

Fig. 10:
Case 3. Septic arthritis of the pubic symphysis caused by Staphylococcus aureus...

Fig. 9:
Case 3. Septic arthritis of the pubic symphysis caused by Staphylococcus aureus...

Fig. 11:
Case 3. Contrast-enhanced coronal CT. Erosions with space widening.

Fig. 15:
Case 3. Septic arthritis of the pubic symphysis caused by Staphylococcus aureus...

Fig. 24:
Case 4. - The collection was drained. Image shows catheter extreme located at...

Fig. 23:
Case 4. - Signs of septic arthritis of the pubic symphysis, with erosions that...

Fig. 22:
Case 4. - Signs of septic arthritis of the pubic symphysis.
It identifies one...

Fig. 21:
Case 4. - Signs of septic arthritis of the pubic symphysis, with lower...

Fig. 20:
Case 4. - Signs of septic arthritis of the pubic symphysis, with left...

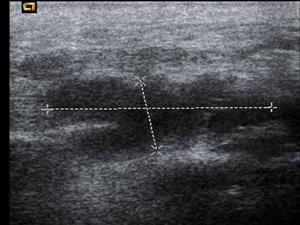
Fig. 19:
Case 4. - Ultrasound at the left inguinal region shows sof tissue abscesified...

Fig. 18:
Case 4. - 61 year old woman
Distension of the joint capsule of the symphysis...

Fig. 17:
Case 4. - 61 year old woman
Distension of the joint capsule of the symphysis...

Fig. 16:
Case 4. - Septic arthritis of the symphysis pubis in a 61 year old...

Fig. 25:
Case 4. Pelvis x-ray. Pubic symphysis diastasis and erosive lesions secondary...

Fig. 33:
Case 5. - 45 year old male patient. Septic arthritis at the pubic symphisis...

Fig. 34:
Case 5. - 45 year old male patient.
Pubic septic arthritis with periarticular...

Fig. 35:
Case 5. - 45 year old male patient.Pubic septic arthritis.

Fig. 36:
Case 5. - 45 year old male patient.
Axial CT scan shows postsurgical changes...

Fig. 32:
Case 5. - 45 year old male patient.
Septic arthritis pubic with distension of...

Fig. 31:
Case 5. - 45 year old male patient.
Septic arthritis with distension of the...

Fig. 30:
Case 5. - 45 year old male.
Septic arthritis of the pubic symphysis
Axial CT...

Fig. 29:
Case 5. - 45 year old male patient.
Septic arthritis with distension of the...

Fig. 28:
Case 5. - 45 year old male patient.
Radiography of pelvis with pubic diastasis...

Fig. 27:
Case 5. - 45 year old male patient.
Ultrasound soft tissue collection reports...

Fig. 26:
Case 5. - 45 year old male patient.
Retrograde cystourethrography reports...

Fig. 37:
Case 5. 45-years-old man.
Radiograph pelvis shows sclerosis and marginal...