ECR 2013 / C-2631
Upper Extremity Venous Ultrasound Doppler: Clinical Perspectives, Technical Procedures and Pictorial Review
Congress:
ECR 2013
Poster Number:
C-2631
Type:
Educational Exhibit
Keywords:
Haemodynamics / Flow dynamics, Diagnostic procedure, Ultrasound-Spectral Doppler, Ultrasound-Colour Doppler, Ultrasound, Vascular, Extremities
Authors:
E. M. Abreu, M. A. E. C. Vasconcelos, M. Palmeiro, J. Niza, A. Loureiro, J. M. Ferreira; Lisboa/PT
DOI:
10.1594/ecr2013/C-2631

Table 1:
Factors increasing risk for upper extremity deep vein thrombosis.

Table 2:
Signs of upper extremity deep vein thrombosis.

Table 3:
Symptoms of upper extremity deep vein thrombosis.

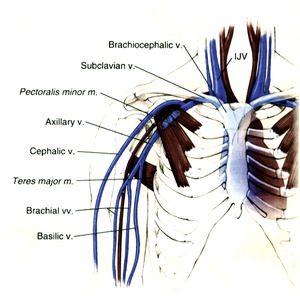
Fig. 1:
Schematic drawing demonstrating venous anatomy of the upper extremity.

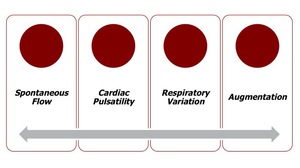
Fig. 2:
Schematic image showing the spectral-Doppler findings.

Table 4:
Diagnostic criteria of upper extremity deep vein thrombosis. Normal findings.

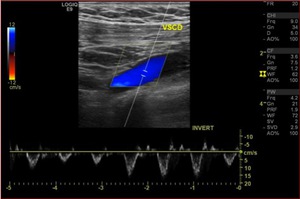
Fig. 3:
Triplex sonogram of the right subclavian vein. In addition to the rapid phasic...

Table 5:
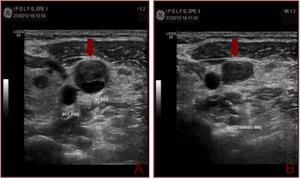
Diagnostic criteria of upper extremity deep vein thrombosis. Non obstructive...
 in the transverse view shows some echogenic material within it (a). Probe pressure is being exerted over the vein (b) and the thrombus is preventing the compression of the vein. This is the key to positively identifying the presence of this non-occlusive thrombus within the vein.")
Fig. 4:
Gray-scale sonogram of the left internal jugular vein (arrows) in the...

Table 6:
Diagnostic criteria of upper extremity deep vein thrombosis. Obstructive...

Fig. 5:
Triplex sonogram in the longitudinal view shows an occlusive thrombus in the...
, in the setting of slow flow. Compression will confirm the complete coaptation of the vessel wall.")
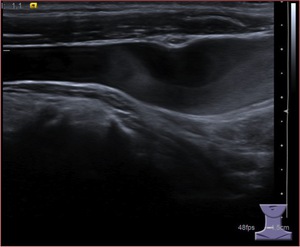
Fig. 6:
Gray-scale sonogram in the longitudinal view shows an area of slow flow in the...
 in the transverse view shows complete colapse of the right vein (a), confirming the absence of thrombus in the examined segment.
The left internal jugular vein shows some echogenic material within it. Note the lack of compression consistent with deep venous thrombosis (b).")
Fig. 7:
US Doppler of a 66-year-old woman with breast cancer.
Gray-scale sonogram of...
.
Note the reduced color flow and almost absence of spectral waveform in the left internal jugular vein, consistent with thrombosis (e).
Although left axillary vein shows color flow, Doppler waveform obtained reveals damping of cardiac and respiratory phasic changes (f). These are indirect findings suggesting the presence of a left brachiocephalic venous thrombus.")
Fig. 8:
US Doppler of a 66-year-old woman with breast cancer.
Triplex sonogram in the...
, consistent with deep venous thrombosis in the left vein.
Note the presence of a central venous catheter portion in the left brachiocephalic vein, surrounded by a venous thrombus (h), confirming that Doppler findings reveal not only direct signs of thrombus in the left jugular vein, but also predict the presence of a clot in non accessible vessels.")
Fig. 9:
CT scan of a 66-year-old woman with breast cancer.
Axial CT scan of thorax...
. The distal tip of the catheter is in superior vena cava (arrow).")
Fig. 10:
Chest radiograph of a middle-aged women with deep venous thrombosis. ...
.
The left internal jugular vein shows some echogenic material, consistent with an occlusive thrombus (d). Although left axillary vein shows color flow, Doppler waveform obtained reveals damping of cardiac and of some respiratory phasic changes, suggesting the presence of a left brachiocephalic venous thrombus (e).")
Fig. 11:
US Doppler of a middle-aged women with deep venous thrombosis.
Triplex...
, confirming that Doppler findings reveal not only direct signs of thrombus in the left jugular vein, but also predict the presence of a clot in non accessible vessels (f,g).")
Fig. 12:
CT scan of a middle-aged women with deep venous thrombosis. ...
, confirming the absence of thrombus in these segments (a,b).")
Fig. 13:
US Doppler of a middle-aged man with inversion of flow direction in the left...
.
Note the abnormal inversion of flow direction in the left internal jugular vein and the pattern of the spectral Doppler waveform (a, c and v-waves) (e).")
Fig. 14:
US Doppler of a middle-aged man with inversion of flow direction in the left...
.")
Fig. 15:
CT scan of a middle-aged man with inversion of flow direction in the left...
 reveal echogenic material within left internal jugular vein. On compression the walls cannot be brought together, due to the thrombus.")
Fig. 16:
US Doppler of a man with laryngeal carcinoma previously submitted to surgery....
.
Although left internal jugular vein shows color flow, Doppler waveform obtained reveals damping of cardiac and respiratory phasic changes (d) due to the presence of a clot in the caudal portion of the vein. Note the reduction of either color flow or spectral waveform in the left axillary vein (e).")
Fig. 17:
US Doppler of a man with laryngeal carcinoma previously submitted to surgery....
 and a mediastinal mass with central necrosis, evolving the left brachiocephalic vein. Note the presence of concomitant pleural metastasis and the left pleural effusion.")
Fig. 18:
CT scan of a man with laryngeal carcinoma previously submitted to surgery....
 in the transverse view shows complete colapse of the right vein, confirming the absence of thrombus in the examined segment (a).
The left internal jugular vein shows echogenic material within it. On compression the walls cannot be brought together, due to the thrombus (b). Gray-sonogram of the left internal jugular vein in the longitudinal view is shown (c).")
Fig. 19:
US Doppler of a man with deep venous thrombosis in the left internal jugular...
.
Although left internal jugular vein shows color flow, Doppler waveform obtained reveals damping of cardiac and respiratory phasic changes, because of the presence of a thrombus in the caudal portion of the vein (e).")
Fig. 20:
US Doppler of a man with deep venous thrombosis in the left internal jugular...
. Note that the spectral analysis confirm the absence of a normal flow, consistent with deep venous thrombosis. (c).
The US Doppler was performed after the treatment, revealing a thrombus-free lumen. The patient still alive after 5 years.")
Fig. 21:
US Doppler of a woman with diffuse large B cell lymphoma.
Gray-scale sonogram...
 and in the longitudinal view (c) show echogenic material within it. On compression the walls cannot be brought together, due to the clot.
Triplex sonogram in the longitudinal plane demonstrates a small area of early recanalization (d). Note the absence of a spectral waveform, consistent with thrombosis (e).")
Fig. 22:
US Doppler of a women with breast cancer, using a central venous catheter for...
. Triplex sonogram in the longitudinal plane of right brachiocephalic vein shows absence of color flow and absence of a spectral waveform (g).")
Fig. 23:
US Doppler of a women with breast cancer, using a central venous catheter for...
.")
Fig. 24:
US Doppler of a women with breast cancer, using a central venous catheter for...
.
Note the echogenic material and absence of flow due to a clot, observed in the triplex scan (n).
The left brachiocephalic vein is patent (o).")
Fig. 25:
US Doppler of a women with breast cancer, using a central venous catheter for...

Note the heterogeneous texture of the thrombus in the left internal jugular vein, that demonstrates areas of recanalization (a).")
Fig. 26:
US Doppler of a middle-aged man complaining of vague neck discomfort and left...
.
Triplex scan in the longitudinal view revealed venous and arterial vascularization of a tumor thrombus infiltrating the vein lumen (b). The CT scan of the thorax revealed tumor thrombus extension until right atrium and multiple pulmonary metastasis. The patient died few months later.")
Fig. 27:
US Doppler of a woman with a poorly differentiated carcinoma of unknown primary...