
ECR 2013 / C-2649
'I GO FOR' (IG4) Autoimmune pancreatitis (AIP) and extra-pancreatic imaging features.
Congress:
ECR 2013
Poster Number:
C-2649
Type:
Educational Exhibit
Keywords:
Abdomen, Pancreas, CT, MR, Ultrasound, Diagnostic procedure, Inflammation
Authors:
R. P. Patel1, T. M. Chandler1, S. Barrett2, J. Coyle3, C. Zwirewich1, A. Harris4; 1Vancouver, BC/CA, 2Dublin /IE, 3Cork/IE, 4BC/CA
DOI:
10.1594/ecr2013/C-2649

Fig. 1:
CECT axial CT in 62 yo female with AIP. Pancreas diffusely enlarged with a...
 in 62 yo female with AIP.")
Fig. 2:
Grayscale USS showing diffusely enlarged hypoechoic gland with ‘sausage’...

Fig. 3:
Follow up imaging in the same patient after steroid treatment. The diffuse...
.")
Fig. 4:
Initial contrast-enhanced CT in a 65 year old male with AIP. The pancreas is...

Fig. 5:
Follow up imaging after a course of steroid treatment. The pancreas has...

Fig. 6:
Axial CECT in a 55 yo man presenting with epigastric pain and jaundice. ...
 and proximal intrahepatic biliary duct dilatation.")
Fig. 7:
Coronal CECT in the same 55yo patient which demonstrates CBD wall enhancement,...
.")
Fig. 8:
ERCP of 55 yo man which shows distal CBD stricture (arrow).
, biliary stent in situ. Adenocarcinoma and focal AIP are often indistinguishable as illustrated. Radiologists need to know about this form of AIP in order to prevent invasive treatment. This patient underwent a Whipple procedure and AIP was diagnosed at pathology.")
Fig. 9:
CECT 55 yo male with focal hypodense mass in the pancreatic head (arrow),...

Fig. 10:
Axial T2 MR 61 yo male with a a focal T2 hypointense mass in the pancreatic...
.")
Fig. 11:
Axial CECT 61 yo old male shows mildly hypoattenuating focal pancreatic head...

Fig. 12:
Focal AIP in 61 yo axial T2 MR, note the mild associated upstream pancreatic...

Fig. 13:
Focal AIP in 61 yo axial CECT, note the mild upstream pancreatic duct...
. Mild upstream main pancreatic duct dilatation and parenchymal atrophy.")
Fig. 14:
MRCP coronal T2 from the same 61 yo patient demonstrated the focal mass in the...
.")
Fig. 15:
ERCP in the 61 yo patient, demonstrates marked narrowing of the intrapancreatic...
 relative to the rest of the pancreas in a 51 yo with Serology and biopsy proven AIP.")
Fig. 16:
Axial CECT showing focal hypoattenuating enlarged pancreatic body (arrow)...
 and resolution of appearances in 51 yo with AIP following steroid treatment.")
Fig. 17:
Axial CECT showing normal homogenous pancreatic enhancement (arrow) and...
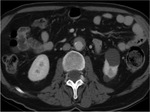
Fig. 18:
Axial CECT in a 65 yo with AIP. A rind of soft tissue is seen surrounding the...
.")
Fig. 19:
Axial CECT post steroid treatment in 65 yo with AIP. The previously seen...
 and an inflammatory abdominal aortic aneurysm (AAA). Note the CBD wall enhancement, thickening and CBD dilatation.")
Fig. 20:
Coronal CECT in a 55 yo man with AIP. There is peri-aortic soft tissue (arrow)...
. These appear as wedge shaped hypodense areas which could be confused with pyelonephritis or other pathology.")
Fig. 21:
Axial CECT 65 yo male with AIP and bilateral renal masses (arrows). These...

Fig. 22:
Axial CECT of the same 65 yo patient with AIP following steroid treatment...

Fig. 23:
Axial CECT in a 59 yo man with AIP and biliary dilatation. Note the dilated...
. A biliary stent is in situ.")
Fig. 24:
Axial CECT in a 59 yo man with AIP and biliary dilatation. Note the degree of...
. Cytologic brushings revealed a diagnosis of autoimmune pancreatitis rather than the expected PSC.")
Fig. 25:
ERCP image from the same 59 yo male with presumed PSC. The CBD has been...

Fig. 26:
Axial CECT in a 57 yo male with AIP. The prostate is diffusely enlarged,...
 revealed abundant IgG4 bearing plasma cells.")
Fig. 27:
Color doppler transverse image of enlarged lymph nodes in the submandibular...
 which has a heterogeneous appearance containing multiple hypoechoic nodules. FNA proven IgG4 rich plasma cells were found in the specimen.")
Fig. 28:
Grayscale image of only the left parotid gland (although bilateral parotid...

Fig. 29:
Color doppler image of only the left parotid gland which has an heterogeneous...