PELVIC BONE STRUCTURE
The bony pelvis consists of innominate bones,
each with three parts (ilium,
isquium and pubis),
sacrum and coccyx.
It protects the pelvic viscera,
provides attachment for the muscles of the trunk and lower limb,
and enables stable transfer of the body weight from the spine to the femora (Figure 1).
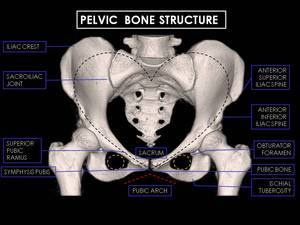
Fig. 1: 3D CT Reconstructions of female pelvis. Note characteristic particularities of female pelvic bone: Heart-shaped pelvic inlet with pelvic outlet (dashed black line), pubic arch angle greater than 90 degrees (dashed red line), round obturator foramen (dashed yellow line), larger and thicker bones.
Its divided into false (major) and true (minior) pelvis, by the ileopectineal line: the smaller inferior part is the true pelvis and the larger superior part is the false pelvis. The false pelvis is formed mainly by the iliac fossae and is largely filled by the iliopsoas muscles.
The true pelvis is bounded posteriorly by the sacrum and coccyx,
laterally by the obturator membranes,
sacrospinous ligaments,
and anteriorly by the pubic bones (Figure 2).
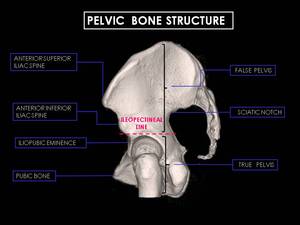
Fig. 2: 3D CT Reconstructions of female pelvis viewed from the medial surface. The ileopectineal line (dashed pink line) is a bony prominence, wich courses from the sacral promontory anteriorly towards the iliopubic eminence. The false pelvis is above the ileopectineal line, while the true pelvis is below it.
The superior aperture of the pelvis is continuous with the abdominal cavity.
The inferior aperture opens to the perineum through the greater sciatic notch and the obturator foramen,
wich are bounded by the coccyx,
pubic symphysis and sacrotuberous ligaments.
PELVIC MUSCULATURE
Anterior Pelvic Wall
The anterior pelvic wall is formed by three flat muscles and the rectus abdominis muscle; all of them continuation of the abdominal wall (Figure 3,4).
1.
External oblique muscle
Largest and most superficial flat muscle
2.
Internal oblique muscle
Middle flat muscle
3. Transversus abdiminis muscle
Inner flat muscle
4.
Rectus abdominis muscle
Vertically directed strap muscle
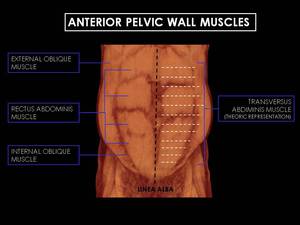
Fig. 3: 3D CT Reconstructions of male anterior abdominal wall. The anterior pelvic wall is formed by three flat muscles and the rectus abdominis muscle; all of them continuation of the abdominal wall. The course transversus abdiminis muscle, the inner pelvic wall muscle, is represented by dashed white lines.
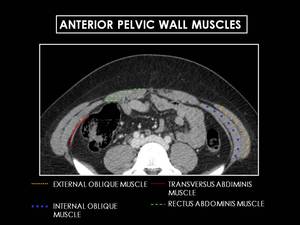
Fig. 4: Axial CT image of female pelvis. The flat muscles that form the lateral anterior abdominal wall include (from external to
internal) the external oblique (yellow dashed lines), internal oblique (blue points) and transversus abdominis muscles (red line). The rectus abdominis muscles are paired, verticallv oriented, strap-like muscle, running on either side of the midline (green dashed lines).
Posterior Pelvic Wall
It is formed by the psoas and iliacus muscles,
which fuse caudally and form the iliopsoas.
The psoas major originates along the lateral surfaces of the  vertebral bodies of T12 and L1-L5 and their associated intervertebral discs.
The iliacus originates in the iliac fossa of the pelvis (Figure 5,6).
vertebral bodies of T12 and L1-L5 and their associated intervertebral discs.
The iliacus originates in the iliac fossa of the pelvis (Figure 5,6).
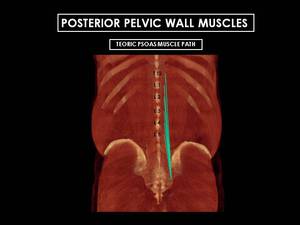
Fig. 5: 3D CT Reconstructions of male posterior abdominal wall. Posterior pelvic wall is formed by the psoas and iliacus muscles, which fuse caudally and form the iliopsoas. The psoas major (represente by green lines) originates along the lateral surfaces of the vertebral bodies of T12 and L1 to L5 and their associated intervertebral discs.
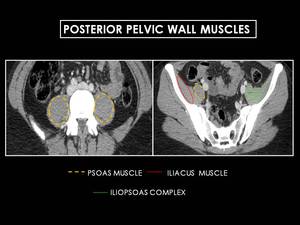
Fig. 6: Axial CT image of female pelvis. The psoas and iliacus muscles merge to form the iliopsoas complex, which continues
inferiorly to insert on the lesser trochanter and serves as a powerful hip flexor.
Pelvic Floor
A strong resistant pelvic floor is necessary to maintain the pelvic viscera in proper position.
This supporting hammock - the pelvic diaphragm - is composed by three key muscles (Figure 7).
Levator ani
- Formed by the pubococcygeous,
iliococcygeous and puborectalis
- Covered by fascial sheath
- Primary support for pelvic organs
- Critical for maintaining continence,
as well as normal micturition and defecation
Coccygeus
- Runs from ischial spine to sacrum and coccyx
Obturator Internus
- Runs from inner surface of obturator membrane to greater trochanter
- Covered by thick fascia (arcus tendineus),
which is origin of pelvic diaphragm
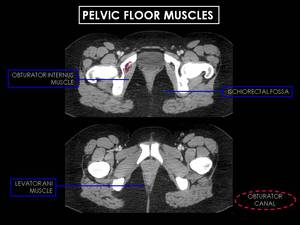
Fig. 7: Pelvic floor muscles. The pelvic diaphragm is composed by three key muscles: levator ani (formed by the pubococcygeous, iliococcygeous and puborectalis), coccygeus (not represented) and obturator internus. The portion of the obturator internus above this origin lies in the lateral wall of the false pelvis, whereas the lower portion forms part of the lateral wall of the ischiorectal fossa.
TEACHING POINT
An important anatomic landmark in CT evaluation of the pelvis is the obturator internus muscle:
- The portion of the obturator internus above this origin lies in the lateral wall of the false pelvis,
whereas the lower portion forms part of the lateral wall of the ischiorectal fossa.
- Between the anal canal and the urogenital diaphragm lies the central tendon of the perineum.
This fibromuscular node is important as the central junction of most of the perineal muscles.
PERITONEUM AND VISCERAL SPACES(Figure 8,9).
The peritoneum is a fibroelastic serous membrane that divides the pelvic cavity in extra and intraperitoneal visceral spaces.
It looks like a closed sac in the male.
In the female,
the ostia of the fallopian tubes allow it to communicate with the outside.
The peritoneal covering of the ovary is intact except during ovulation when rupture of the membrane occurs allowing an oocyte to pass into the peritoneal space and proceed to the ostium of the fallopian tube.
The inferior recesses of the peritoneal cavity usually do not project bellow the level of the mid portion of the femoral heads.
In the male pelvis,
the peritoneum sweeps anteriorly from the frontal surface of the rectum to the posterior aspect of the bladder and superiorly to the seminal vesicles forming the rectovesical pouch.
In the female,
the uterus intervenes between the rectum and bladder forming a recto-uterine pouch as well as the utero-vesical pouch anteriorly.
Intraperitoneal Spaces
Paravesical Left And Right Spaces
With their principal stamps:
- The median umbilical ligament or urachus,
the embryological remnant of the umbilical artery extending from the bladder dome to navel.
- The lateral umbilical ligament,
which medially limits the paravesical space and the inguinal fossa laterally.
Posterior Bladder Spaces
Varies from men to women:
- In men we see recto-vesical space.
- In women,
we see anterior utero-vesical pouch and posterior recto-uterine pouch or pouch of Douglas.
TEACHING POINT
Rectovesical pouch is most dependent recess in men
Vesicouterine pouch and rectouterine (of Douglas)
are most dependent in women
Extraperitoneal Spaces
Retropubic prevesical space.
Separated from anterior abdominal wall by the transversals fascia.
Located between the umbilico-vesical fascia and peritoneum.
It contains the bladder,
umbilical arteries and the urachus.
It is located between rectum and sacrum/coccyx and contains autonomic nerves from pelvic viscera.
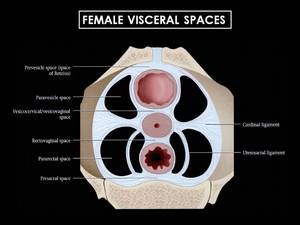
Fig. 8: Schematic representation of the ligaments and spaces at the cervical/vaginal junction. The ligaments are visceral ligaments, which are composed of specialized endopelvic fascia and contain vessels, nerves and lymphatics. The main supporting ligaments for the uterus are the cardinal and uterosacral ligaments. (Source - Diagnostic and Surgical Imaging Anatomy. Michael Federle. Page 1051 -).
References: (Source - Diagnostic and Surgical Imaging Anatomy. Michael Federle. Page 1051 -)
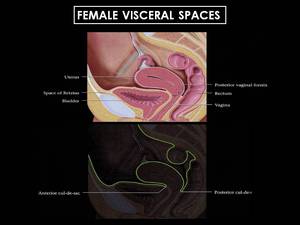
Fig. 9: Sagittal graphic of the female pelvis shows the bladder, uterus and rectum, all of wich are extraperitoneal. The peritoneum has been highlighted to show the cul-de sacs. Posteriorly, the peritoneum extends along the posterior vaginal fornix, creating the posterior cul-de-sac (pouch of Douglas), the most dependent portion of the pelvis. Anteriorly, at the level of the lower uterine segment, the peritoneum is reflected over the dome of the bladder, creating the anterior cul-de-sac. (Source - Diagnostic and Surgical Imaging Anatomy. Michael Federle. Page 1053 -).
References: (Source - Diagnostic and Surgical Imaging Anatomy. Michael Federle. Page 1053 -).
PELVIC VESSELS (Figures 10,11)
Arterial System Key Points
Abdominal Aorta
- Divides into common iliac arteries at t L4-L5 level.
- Testicular and ovarian arteries originate below renal arteries.
Common iliac arteries
- Run anterior iliac veins and inferior to vena cava.
- Descend behind the ureters.
- Divides into external and internal iliac arteries at the sacroiliac joint level.
Internal iliac artery (hypograstric)
- Principal vascular support of pelvic organs
- Descends toward the greater sciatic notch
- Divides into anterior and posterior trunk
- Anterior trunk to pelvic viscera.
- Posterior trunk to pelvic musculature
External iliac artery
- Exits pelvic beneath inguinal ligament
- Inferior epigastric (medial) and deep iliac circumflex (lateral) arteries demarcate junction between external iliac and common femoral arteries.
Pelvic Veins Key Points
The external and internal iliac veins correspond to their arteries.
They have a medial position with respect to the arteries and becoming posterior progressively.
External iliac vein
- Upward continuation of femoral vein at level of inguinal ligament
Internal iliac vein
- Begins near upper part of greater sciatic foramen
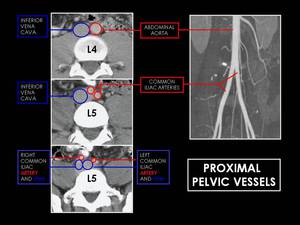
Fig. 10: Axial CT images at L4/L5 level in portal fase and MIP angio TC reconstruction. Note how the abdominal aorta divides into common iliac arteries at L4-L5 level and how after these division these vessels run anterior iliac veins and inferior to vena cava.
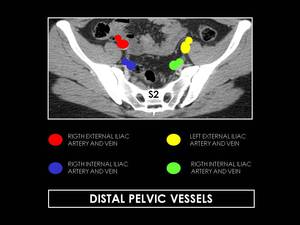
Fig. 11: Axial CT images at S2 level showing distal pelvic vessels. The common iliac arteries divide, at the level of L5-S1, into two branches, the external and internal iliac (hypogastric) arteries. The external iliac artery supplies the lower extremity, while the hypogastric artery supplies the pelvic viscera and muscles of the pelvis.
TEACHING POINT
Right gonadal vein drains into vena cava
Left gonadal vein drains into left renal vein
PELVIC STRUCTURES OF THE DIGESTIVE TRACT (Figure 12)
Sigmoid Colon
- Variable length and morphology.
- Supplied by the inferior mesenteric artery and vein.
- Coated by a double layer of peritoneum.
Rectum
- Final 15-20 cm of colon.
- Rectosigmoid junction at lumbo-sacral level (variable).
- Lies in extraperitoneal pelvis
- It has mesenteric and systemic vessels: Superior rectal branches of inferior mesenteric artery and vein and middle and inferior rectal braches of internal iliac vessels.
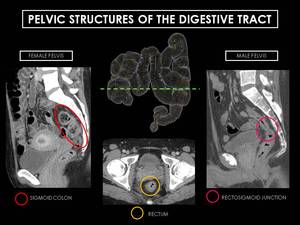
Fig. 12: Sagittal CT images at S2 level showing pelvic structures of the digestive tract. The green dashed line divides the pelvic colon structures from abdominal portion. Note the relationship between the male and female pelvic structures as the rectosigmoid junction is sacral level.
LOWER URINARY TRACT STRUCTURES (Figure 13)
Pelvic Ureters
- Distal ureters enter the pelvis in front of the psoas muscle.
- Lie along pelvic lateral walls near internal iliac vessels.
- At the level of inferior iliac spines ureters curve anteromedially to enter bladder at level of seminal vesicles in men and cervix in women.
- Ureterovesical junction: Ureters pass obliquely through muscular wall of bladder crating a valve effect.
Bladder
Lies in extraperitoneal (retroperitoneal) pelvis.
Surrounded by loose connective tissue and fat.
- Perivesical space: contains bladder and urachus.
- Prevesical space (Retzius): between bladder and symphysis pubis.
Peritoneum covers dome of bladder.
- Rectovesical pouch is most dependent recess in men
- Vesicouterine pouch and rectouterine (of Douglas) are most dependent in women.
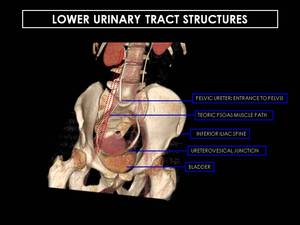
Fig. 13: Coronal reformatted CT urogram. Distal ureters enter the pelvis in front of the psoas muscle.Note how at inferior iliac spine level ureters curve anteromedially to enter bladder at level of seminal vesicles in men and cervix in women.
MALE PELVIC STRUCTURES (Figure 14)
Prostate
Wal-nut sized gland located beneath bladder and in front of the rectum.
It is above superior fascia of urogenital diaphragm and surrounds the uppermost part of the urethra.
Its normal size is between 3 x 4 x 2cm (CC x TV x L diameters).
Conical in shape with base,
apex and anterior,
posterior and two inferolateral surfaces:
- Base closely related to inferior surface of bladder.
- Apex in contact with superior fascia of urogenital diaphragm.
- Posterior surface separated from rectum by rectovesical septum (Denonvilliers fascia).
- Two ejaculatory ducts enter prostate through posterior surface
- Posterosuperiorly,
seminal vesicles lie between bladder base and rectum.
- Anterior surface separated from symphysis pubis by extraperitoneal fat and plexus of veins and connected to pubic by puboprostatic ligaments.
- Inferolateral surfaces separated from levator ani by periprostatic plexus of veins.
Seminal Vesicles and Ejaculatory Ducts
- SV are saclike structures located superolaterally to prostate,
between fundus of urinary bladder and rectum.
- Ejaculatory Ducts are located on either side of midline,
start at base of prostate and run forward and downward through gland.
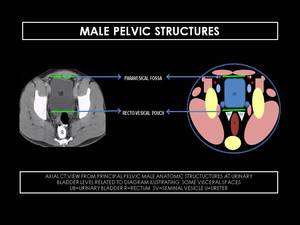
Fig. 14: Axial CT view from principal pelvic male anatomic structures at urinary bladder level.
FEMALE PELVIC STRUCTURES (Figure 15)
Ligaments
Supporting Uterine Ligaments
- These are visceral ligaments and contain vessels neres and lymphatics,
as well connective tissue,
makes a similar function as bowel mesentery and a supportive role connects viscera to pelvic wall.
- Peritoneum extends over bladder dome anterior uterus and reflects over uterurs at lower uterine segment,
creating the anterior cul-de-sac (vesico-uterine pouch).
- Over fundus,
the peritoneum extends over posterior uterine surface to upper vagina,
abutting posterior vaginal fornix,
crating posterior cul-de-sac (pouch of Douglas or rectouterine pouch).
Broad Ligament
- It is created from the two sheets of covering peritoneum and extends laterally to pelvic sidewall covering fallopian tubes.
Ovarian Ligaments
- Suspensory ligament of ovary attaches ovary to pelvic wall an contains ovarian artery and vein.
- Proper ovarian ligament attaches ovary to uterine corpus.
- Mesosalpinx between fallopian tube and proper ovarian ligament.
Round Ligamnets
- Arise from uterine cornu near fallopian tubes.
- Course anteriorly,
through inguinal canal to insert on labia majora
- Offer little support to uterus.
Uterosacral Ligaments
- Extend from cervix and vagina to sacrum.
- Extend around rectum and form lateral borders of pouch of Douglas.
Uterus
Located between the bladder in front and the rectum behind,
it is an extraperitoneal organ.
- Composed of myometrium and endometrium
- It has two major divisions: body and cervix
- Uterine position:
-
- Flexion is axis of uterine body relative to cervix
- Version is axis of cervix relative to vagina
- Most uteri are anteverted and anteflexed
Cervix
- Begins at inferior narrowing of uterus (isthmus).
- It has a supravaginal and vaginal portion.
Fallopian Tubes
- Connects uterus to peritoneal cavity.
- Attached to posterior broad ligament by mesosalpinx.
- Composed of four segments:
-
- Interstitial
- Isthmus,
narrow portion of tube immediately adjacent to uterus.
- Ampulla,
tortuous,
ecstatic portion contiguous with isthmus.
Fertilization usually occurs in this portion of tube.
- Infundibulum,
funnem-shaped opening ringed by finger-like fimbriae.
Vagina
It is an extra-peritoneal structure,
by front is related to the bladder in its most upper region and beneath the urethra.
Its back side is in contact with the pouch of Douglas.
Its both sides contacts with levator ani and urogenital diagragma.
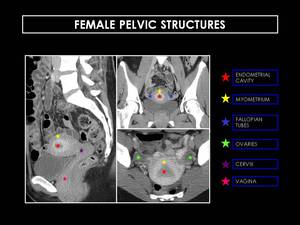
Fig. 15: Sagittal, coronal, and axial CT scan of three different women. Note how the enhancement of the endometrial cavity varies according to factors such as age or the period of reproductive cycle.


, pubic arch angle greater than 90 degrees (dashed red line), round obturator foramen (dashed yellow line), larger and thicker bones.")
 is a bony prominence, wich courses from the sacral promontory anteriorly towards the iliopubic eminence. The false pelvis is above the ileopectineal line, while the true pelvis is below it.")

 the external oblique (yellow dashed lines), internal oblique (blue points) and transversus abdominis muscles (red line). The rectus abdominis muscles are paired, verticallv oriented, strap-like muscle, running on either side of the midline (green dashed lines).")
 originates along the lateral surfaces of the vertebral bodies of T12 and L1 to L5 and their associated intervertebral discs.")

, coccygeus (not represented) and obturator internus. The portion of the obturator internus above this origin lies in the lateral wall of the false pelvis, whereas the lower portion forms part of the lateral wall of the ischiorectal fossa.")
. References: (Source - Diagnostic and Surgical Imaging Anatomy. Michael Federle. Page 1051 -)")
, the most dependent portion of the pelvis. Anteriorly, at the level of the lower uterine segment, the peritoneum is reflected over the dome of the bladder, creating the anterior cul-de-sac. (Source - Diagnostic and Surgical Imaging Anatomy. Michael Federle. Page 1053 -). References: (Source - Diagnostic and Surgical Imaging Anatomy. Michael Federle. Page 1053 -).")

 arteries. The external iliac artery supplies the lower extremity, while the hypogastric artery supplies the pelvic viscera and muscles of the pelvis.")



