ECR 2014 / C-0476
Bursae around the hip: anatomy, pathology, and mimics
This poster is published under an open license. Please read the disclaimer for further details.
Congress:
ECR 2014
Poster Number:
C-0476
Type:
Educational Exhibit
Keywords:
Inflammation, Normal variants, MR, Musculoskeletal soft tissue
Authors:
P. M. E. Souza, E. B. G. D. Santos; Rio de Janeiro/BR
DOI:
10.1594/ecr2014/C-0476

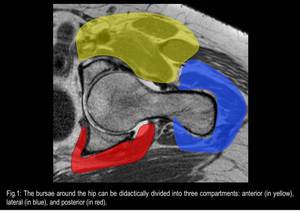
Fig. 1

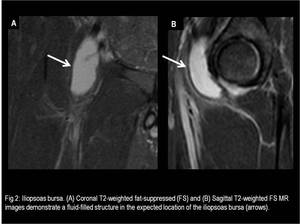
Fig. 2

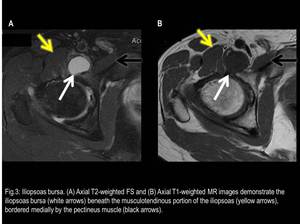
Fig. 3

Fig. 4

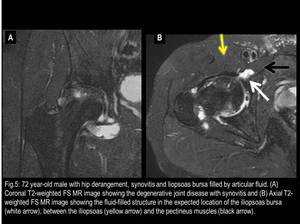
Fig. 5

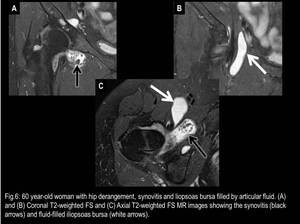
Fig. 6

Fig. 7

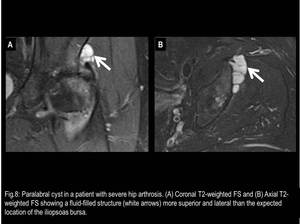
Fig. 8

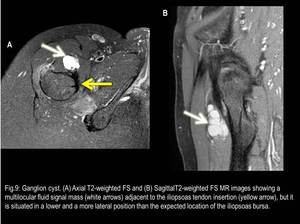
Fig. 9

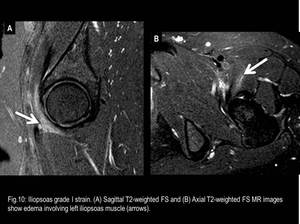
Fig. 10

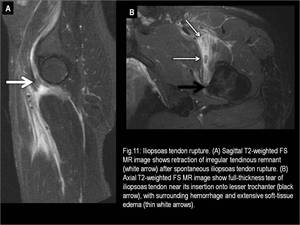
Fig. 11

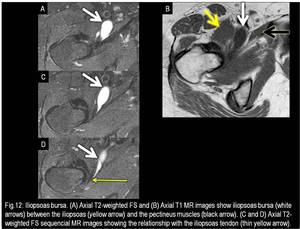
Fig. 12

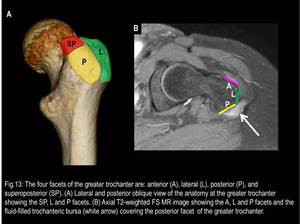
Fig. 13

Fig. 14

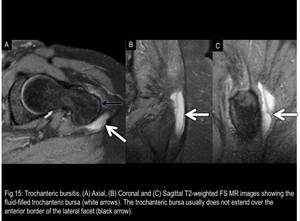
Fig. 15

Fig. 16

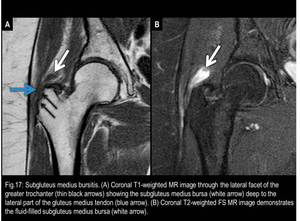
Fig. 17

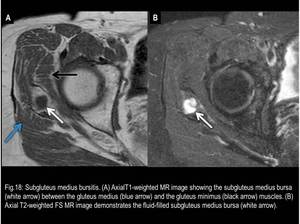
Fig. 18

Fig. 19

Fig. 20

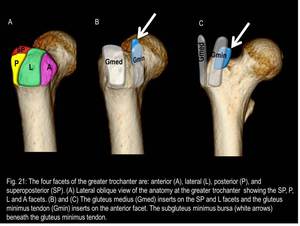
Fig. 21

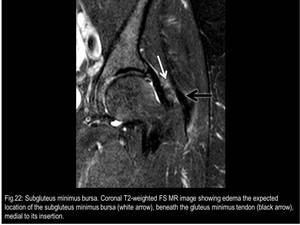
Fig. 22

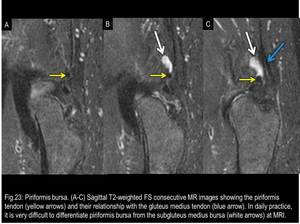
Fig. 23

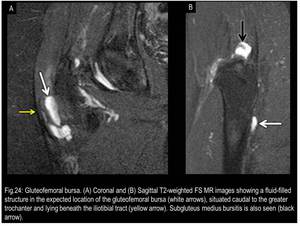
Fig. 24

Fig. 25

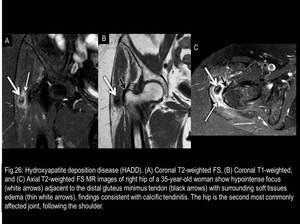
Fig. 26

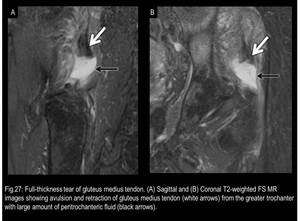
Fig. 27

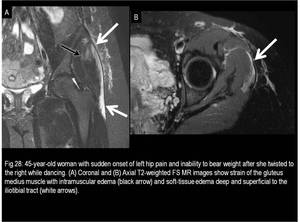
Fig. 28

Fig. 29

Fig. 30

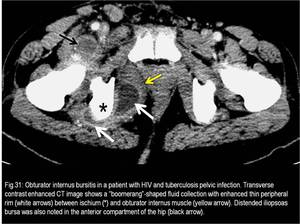
Fig. 31

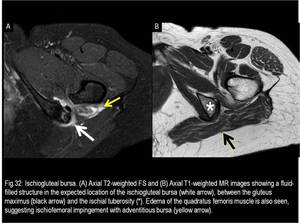
Fig. 32

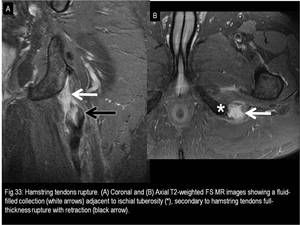
Fig. 33