Ultrasound imaging technique
This examination is routinely performed through the anterior fontanel,
which remains patent in full-term infants until 9-18 months of age and serves as an acoustic window.
In premature infants and in those with increased intracranial pressure,
the anterior fontanel remains patent for a longer time.
Scanning is also possible through the posterior fontanel,
in coronal,
sagittal and oblique planes,
as well as through the squamosal suture,
anterolateral,
posterolatral fontanel and even through bone windows in patients with closed fontanels.
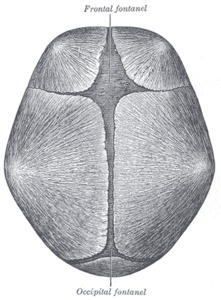
Fig. 1: The skull at birth, showing the anterior and posterior fontanels.
References: www.wikipedia.org
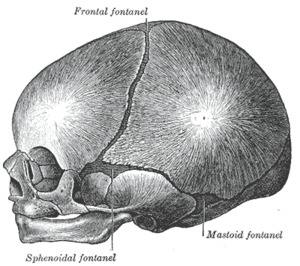
Fig. 2: The skull at birth, showing the lateral fontanels.
References: www.wikipedia.org
The correct choice of the transducer depends on the size of the cranial vault and the sonic windows:
For maximal resolution and depth penetration:
- 9-4 MHz curvilinear transducer is recommended for older babies
- 8-5 MHz small transducer for newborns
- 12-5,
17-5 and 15 MHZ linear transducer for superficial lesions and for the evaluation of the internal content of meningocele or encephalocele.
All the transducer allow the use of duplex/color Doppler imaging.
To scan as much of the intracranial contents as possible,
a sequential scan is necessary:
- from anterior to posterior in the coronal plane
- from the midline to the later aspects in the sagittal plane,
using the ventricular system and the cerebrospinal fluid (CSF) as main references for the identification of anatomical structures.
The parasagittal view of the brain includes the lateral ventricles,
with the corresponding frontal horns and bodies and the caudothalamic groove,
a thin,
echogenic band,
located between the caudate nucleus anteriorly and the thalamus posteriorly.
The highly vascular germinal matrix is found in preterm infants inferolateral to the ependyma lining the floor of the lateral ventricle,
anterior and superior to the caudothalamic groove.
The scan of the lateral ventricles also reaches the bodies and temporal and occipital horns.
Within the atrium of the lateral ventricle,
the choroid plexus can be seen.
Frequently,
the lateral ventricles are asymmetric,
with the occipital horns wider than the frontal ones.
Posterior to the occipital horns,
a periventricular blush of echogenity is found,
supposedly related to white matter fibers and vascular plexus.
Parasagittal views picture the brain in the periventricular region,
the Sylvian fissure and insula.
The midline sagittal scan of the brain is obtained with the transducer parallel to the anteroposterior diameter of the cranial vault.
The cavum septum pellucidum is identified as a fluid-filled structure located between the frontal horns of the lateral ventricles.
Above this midline fluid-filled structure is the corpus callosum,
a thin,
crescent-shaped,
hypoechoic structure with the main components - genu,
body and splenium.
Superiorly to the corpus callosum,
a broad,
curvilinear hypoechoic band,
representing the cingulate gyrus is seen.
It is separated from the more superficial gyri by the cingulate sulcus,
a thin hypoechoic line.
Vascular pulsations of the branches of the anterior cerebral arteries can also be seen within the cerebral sulci,
with real-time imaging.
The third and fourth ventricles are pictured as hypoechoic structures on the midline,
with the bright area of the choroid plexus within the third ventricle.
A dense band,
representing the quadrigeminal plate,
lies behind the third ventricle.
Below this cistern, the brightly echogenic cerebellar vermis is seen, indented anteriorly by the triangular fourth ventricle.
The cisterna magna,
with an anechoic appearance,
is located inferior to the cerebellum and communicates with the fourth ventricle.
The moderately echoic brain stem lies anterior to the fourth ventricle and posterior to the clivus.
Fig. 22: Ultrasound neonatal brain scan - sagittal view
References: Department of Radiology, 3rd Pediatric Clinic, Cluj - Napoca
Coronal plane imaging begins anteriorly and shifts posteriorly.
A first,
far anterior view of the frontal hemispheres should depict the anterior tips of the frontal horns of the lateral ventricles,
the interhemispheric fissure,
and the orbits.
A second image is acquired at the level of the frontal horns or bodies of the lateral ventricles,
anterior to the foramina of Monroe. The anterior horns of the lateral ventricles appear as anechoic,
crescent,
paramedian,
fluid-filled structures. The roof of this portion of the lateral ventricle is formed by the corpus callosum,
the medial walls by the cavum septi pellucidi and the lateral walls,
which normally are concave,
by the heads of the caudate nuclei.
The superior aspect of the corpus callosum is separated from the hypoechoic cingulate gyrus by the brightly hyperechoic pericallosal sulcus. The putamen and globus pallidus are located lateral and inferior to the caudate nucleus. The hypoechoic frontal and temporal lobes are imaged at this level. Vascular pulsations may also be observed with real-time imaging- those of the anterior cerebral arteries in the interhemispheric fissure and those of the middle cerebral arteries in the Sylvian fissure.
The next section is obtained slightly posteriorly at the level of the foramen of Monroe,
where the lateral and third ventricles communicate.
Because of its small size,
the normal third ventricle is not visualized.
Vascular pulsations from the anterior and middle cerebral arteries can also be observed on this scan.
In extension,
the relatively echogenic brains stem - pons and medulla - is observed on this image.
The choroid plexus is seen in the roof of the third ventricle and in the groove between the ventricle and the thalamus.
The next image is acquired at the level of the quadrigeminal plate cistern and the cerebellum.
On this view,
a midline pie-shaped area of bright echogenicity, occupying the lower third of the brain with the
anechoic cisterna magna posteriorly and inferiorly,
represents the cerebellar vermis.
The bodies of the lateral ventricles are seen superiorly and the temporal horns inferiorly.
On this image,
the pulsations of the middle cerebral and pericallosal arteries can be observed.
On the next scan,
at the posterior aspects of the lateral ventricles,
at the level of the trigone,
the choroid plexus is depicted.
The splenium of the corpus callosum separates the lateral ventricles,
as they diverge. Also,
the previously described periventricular blush is seen lateral to the posterior horns of the lateral ventricles.
Inferiorly,
the posterior part of the cerebellum is observed.
The final image is the most posterior view of the brain parenchyma
in the coronal projection and it is important for evaluation of the parenchyma.
It includes the more superficial sulci and gyri of the occipital lobes and the echogenic areas located superior to the atria of the lateral ventricles,
representing white matter.
Fig. 23: Ultrasound neonatal brain scan - coronal view
References: Department of Radiology, 3rd Pediatric Clinic, Cluj - Napoca
The extra-axial fluid space can be most easily visualized ultrasonographically in the midline. For the assessment of the extracerebral spaces,
a high-frequency - 12-15 MHz - transducer is the most suitable.
With this technique,
the extra-axial spaces,
cerebral convexities and extra-axial vessels are accessible to the examiner. Normal measurements include: sinocortical width - 0.4 to 3.3 mm,
craniocortical width - 0.3 to 6.3 mm,
interhemispheric width - 0.5 to 8.2 mm.
Posterior fontanel
Posterior fontanel imaging is recommended for examining posterior fossa abnormalities,
for a greater accuracy in detecting intraventricular hemorrhage (IVH),
for the differentiation between clot and choroid and a better depiction of the occipital and temporal horns.
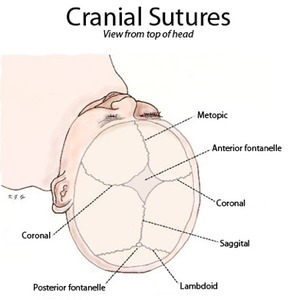
Fig. 3: Cranial sutures shown from top of head.
References: www.wikipedia.org
Mastoid fontanel
When using the mastoid fontanel as an acoustic window,
for assessment of the posterior fossa and brain stem,
a high-frequency transducer is positioned 1 cm posterior to the ear and 1 cm above the tragus.
Images obtained this way are useful in detecting hemorrhage involving the brain stem,
cerebellum and subarachnoid cisterns,
in detection of clot within the fourth ventricle and cisterna magna and in demonstration of posterior fossa malformations.
Color Doppler images
Color Doppler images may be acquired for the screening of the vascular structures.
An image obtained through the anterior or temporal fontanel will provide a picture of the circle of Willis.
Patency and resistance to flow will be appreciated,
but also spectral tracing with measurements of peak systolic velocity (PSV),
end-diastolic velocity (EDV) and resistive index (RI) is possible.
A color Doppler image of the sagittal sinus and vein of Galen,
obtained in the sagittal plane will provide information about the patency of the venous system.
Power-Doppler is useful in areas of hyper- or hypovascularity,
as may occur in vascular occlusion,
ischemia and infarction.
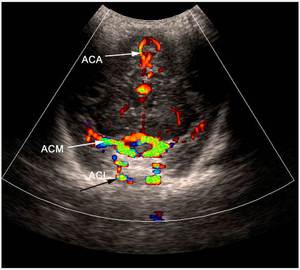
Fig. 5: Coronal section - Willis circle - color Doppler. ACA = anterior cerebral artery, ACM = middle cerebral artery.
References: Department of Radiology, 3rd Pediatric Clinic, Cluj - Napoca
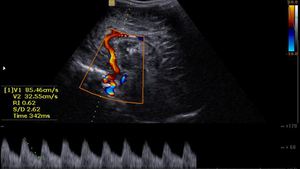
Fig. 21: Sagittal section - Doppler measurements
References: Department of Radiology, 3rd Pediatric Clinic, Cluj - Napoca
Normal variants:
- asymmetry in size of the lateral ventricles,
the left being more often
larger than the right and most pronounced in the most posterior portion of the occipital horn
- coarctation of the lateral ventricles, unilateral or bilateral, may have the appearance of a germinal matrix cyst or periventricular leukomalacia (PVL)
- split choroid - cleft or lobular appearance of the ventricular atrium,
may be confused with choroidal hemorrhage
- truncated choroid plexus - flattening of the rounded lower portion of the plexus
- choroid cyst,
may be single or multiple,
variable in size
Pathological findings
Intracranial hemorrhage
Intracranial hemorrhage represents a leading cause of morbidity and mortality in newborns,
especially in preterm infants.
Risk factors:
- prematurity (less than 32 weeks’ gestation)
- low birth weight (less than 1500 g)
- sex (males 2:1)
- multiple gestations
- trauma at delivery
- prolonged labor
- hypocoagulation
- pneumothorax
- patent ductus arteriosus
- factors associated with increased or decreased cerebral blood flow
ICH in the premature neonate has been divided into four grades,
the most widely accepted classification being modified from that of Papile et al:
grade I - subependymal germinal matrix hemorrhage (GMH);

Fig. 6: Coronal section - grade I - subependymal germinal matrix hemorrhage (blue arrows).
References: Department of Radiology, 3rd Pediatric Clinic, Cluj - Napoca
grade II - GMH and IVH without ventricular dilation;
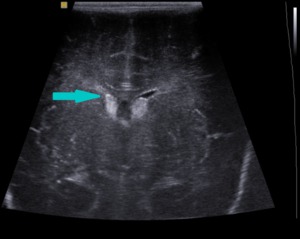
Fig. 7: Coronal section - grade II - GMH and IVH without ventricular dilation (blue arrow).
References: Department of Radiology, 3rd Pediatric Clinic, Cluj - Napoca
grade III - A.
mild GMH and IVH with ventricular dilation;
B.
moderate GMH and IVH with ventricular dilation
C.
severe GMH and IVH with ventricular dilation

Fig. 8: Sagittal section - grade III - GMH and IVH with ventricular dilation (white arrows).
References: Department of Radiology, 3rd Pediatric Clinic, Cluj - Napoca
grade IV - intraparenchymal hemorrhage (IPH) with IVH.
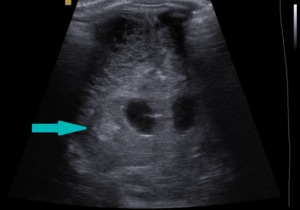
Fig. 9: Coronal section - grade IV- intraparenchymal hemorrhage (blue arrow).
References: Department of Radiology, 3rd Pediatric Clinic, Cluj - Napoca
Ultrasound findings:
The germinal matrix represents a highly cellular, richly vascular,
and metabolically active area,
which lies beneath the ependyma of the lateral ventricles and represents the usual initial site of ICH in the premature brain.
Germinal matrix hemorrhage (GMH):
- appears in the first week of life
- uniformly echogenic mass inferolateral to the frontal horns at a level just posterior to the foramen of Monroe
- may be unilateral or bilateral
- if large,
it can cause focal compression of the inferolateral margin of the ventricle
- typical appearance: round region of asymmetric hyperechogenity.
- if the hemorrhage resolves,
the focal lesion decreases in size an echogenity and frequently results in a subenepndymal cyst.
Intraventricular hemorrhage (IVH):
- may represent the intraventricular extension of GMH
- may be unilateral or bilateral
- bright echoes within the ventricular lumen.
- if the ventricles are not dilated (i.e.,
grade II IVH),
the clot may be difficult to identify and to separate from the choroid plexus
- in grade III IVH with ventricular dilation,
the clot is easily detected.
- with severe hemorrhage, the entire ventricle is filled with blood,
forming a cast of the ventricle.
- as the hemorrhage resolves,
the interior becomes hypoechoic,
surrounded by a echogenic rim
- residual intraventricular septation may persist and a week after the event
- other possible consequences: ventricular enlargement,
posthemorrhagic hydrocephalus,
inflammatory ependimitis
Intraparenchymal hemorrhage (IPH):
- the most severe grade of ICH in the premature infant
- hemorrhage into areas that are already damaged by periventricular leucomalakia (PVL)
- associated with IVH in 80% of cases
- occurs on the side of the cerebral hemisphere with the more severe IVH
- brightly echogenic appearance
- frontoparietal distribution and
- often causes a mass effect.
- resolves in a similar manner with the other types of inctracranial hemorrhage and a porencephalic cyst may form
Other,
much less common sites of ICH in the neonate are subarachnoid hemorrhage (SAH) and intracerebellar hemorrhage (CBH).
Subarachnoid hemorrhage (SAH):
- increased echogenity and widening of the horizontal portion of the Sylvian fissure
- subtle changes,
only detectable with large quantities of blood
- Ct is the preferred imaging modality
Intracerebellar hemorrhage (CBH):
- the use of the mastoid fontanel improves diagnosis
- poor prognosis
- echodense area within the cerebellum
- 4th ventricle not visualized
- on sagittal scans - loss of normal differentiation of the brain stem structures
Subdural and epidural hemorrhages:
- usually occur in term infants secondary to trauma
- enlarged craniocortical distance
- widening of the interhemispheric fissure
- a linear or elliptical fluid collection between the brain and the skull
- mass effect
- CT and magnetic resonance imaging (MRI) are the preferred imaging modalities
Hypoxic-ischemic encephalopathy
Perinatal hypoxic-ischemic injury of the brain induces major neurologic and developmental deficits in infants and young children.
GMH-IHV is the most frequent consequence of a hypoxic brain injury in the preterm infant.
If the ischemic component is also significant,
infarct may occur,
resulting in PVL and periventricular hemorrhagic infarction (PVHI) in the premature infants.
Periventricular leukomalacia (PVL):
- coagulation necrosis of the white matter
- occurs at the external angle of the frontal horns near the foramen of Monroe and at the level of the optic radiations adjacent to the trigone
- bilateral,
coarse,
globular,
or broad bands of echogenity in the periventricular white matter
- bilateral and symmetric pattern
- usually in the first 10 days of life
- evolves to multiple tiny cysts or porencephalic cysts
- white-matter gliotic scars
- ventricular enlargement
- MRI represents a useful diagnostic adjunct
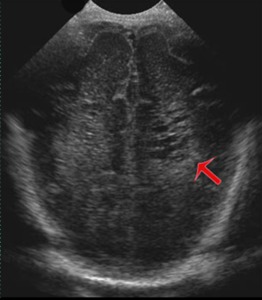
Fig. 10: Coronal section - Periventricular leukomalacia (red arrow) - cystic transformation.
References: Department of Radiology, 3rd Pediatric Clinic, Cluj - Napoca
Periventricular hemorrhagic infarction (PVHI):
- area of hemorrhagic necrosis in the periventricular white matter
- dorsal and lateral to the external angle of the lateral ventricle
- unilateral or bilateral
- asymmetric,
globular or triangular fan-shaped echogenic lesion,
radiating from the external angle of the lateral ventricle
- localized or extensive in the periventricular white matter
- evolves into cystic cavities,
usually single and large and progress to porencephaly
- poor prognosis
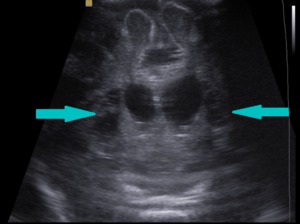
Fig. 11: Coronal section - Periventricular hemorrhagic infarction with cystic transformation (blue arrows).
References: Department of Radiology, 3rd Pediatric Clinic, Cluj - Napoca
Perinatal asphyxia:
- term infant
- tiny slit-like ventricles
- obliteration of the extra-axial fluid spaces
- hazy increased parenchymal echogenicity
Cerebral cortical infarction:
- rare condition
- risk factors: prematurity, asphyxia,
congenital heart disease,
polycythemia and hyperviscosity,
trauma,
meningitis,
and thromboembolism
- common involvement of the middle cerebral artery distribution
- absence of gyral definition
- absence of vascular pulsations
- altered parenchymal echogenicity
Congenital anomalies
Hydrocephalus:
- the most common congenital anomaly in neonates
- increased volume of fluid within the ventricular
- can be either obstructive or nonobstructive
- obstructive hydrocephalus can be classified as noncommunicating,
in which the point of obstruction occurs within the ventricular system and communicating,
in which the obstruction occurs beyond the ventricular system,
the arachnoid granulations.
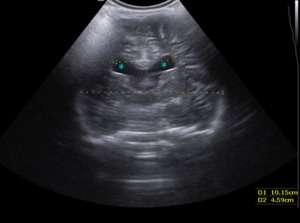
Fig. 12: Coronal section - Hydrocephalus with little ventricular dilation (blue stars).
References: Department of Radiology, 3rd Pediatric Clinic, Cluj - Napoca
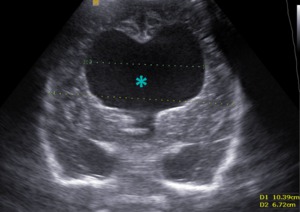
Fig. 13: Coronal section - Large hydrocephalus (blue star).
References: Department of Radiology, 3rd Pediatric Clinic, Cluj - Napoca
Disorders of closure
Skull defects,
also known as “cranium bifidum,” are often associated with congenital malformations of the brain,
meninges,
or both.
These
defects most often present as a midline occipital mass.
Meningocele:
- small defect
- only meninges herniate
Encephalomeningocele:
- the defect is large
- the meninges and part of the brain herniate
Meningohydroencephalocele:
- the brain tissue herniates along with a portion of the ventricle and meninges

Fig. 4: Illustration of a child with encephalocele
References: www.wikipedia.org
The corpus callosum is the largest structure which connects the two hemispheres.
Primary agenesis:
- occurs around the 12th gestational week
- associates lipoma,
encephalocele,
arachnoid cyst or migrational abnormality
Secondary dysgenesis:
- occurs later,
due to destruction of previously formed corpus callosum - associates microcephaly, Dandy–Walker syndrome,
Arnold–Chiari malformation,
holoprosencephaly,
cyclopia,
septo-optic dysplasia,
porencephaly or aqueductal stenosis.
Ultrasound findings:
- absence of sonolucent band in location of corpus callosum
- widely separated frontal horns and bodies of lateral ventricles
- colpocephaly
- concave medial borders of lateral ventricles
- dilation and posterosuperior displacement of third ventricles
- radial arrangement of medial cerebral sulci.
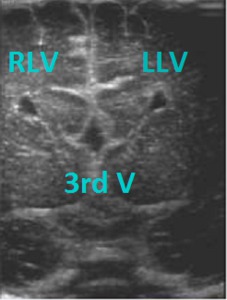
Fig. 14: Coronal section - Absent corpus callosum, widely separated frontal horns of lateral ventricles, dilation and posterosuperior displacement of third ventricle.
References: Department of Radiology, 3rd Pediatric Clinic, Cluj - Napoca
Dandy-Walker cysts:
- cystic dilation of the fourth ventricle
- hypoplastic cerebellar hemispheres
- absent or rudimentary vermis
- large posterior fossa continuous with the fourth ventricle
- variable degrees of hydrocephalus
- associated with encephalocele,
agenesis of the corpus callosum,
holoprosencephaly,
gyral anomalies,
heterotopias,
cleft palate,
polysyndactylism.
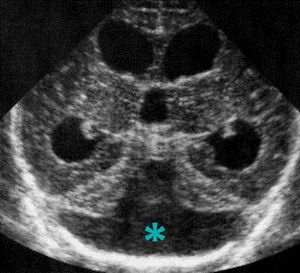
Fig. 15: Coronal section - Dandy - Walker malformation - dilation of the fourth ventricle (blue star), hypoplastic cerebellar hemispheres.
References: Department of Radiology, 3rd Pediatric Clinic, Cluj - Napoca
Arnold- Chiari type I:
- inferior displacement of the tonsils and cerebellum
- no displacement of the fourth ventricle or the medulla
Arnold–Chiari type II:
- the most common type seen in neonates and infants
- small posterior fossa
- downward displacement of medulla,
forth ventricle,
cerebellum
- obliteration of cisterna magna
- elongation of pons and fourth ventricle
- hydrocephalus
- colpocephaly
- dilation of the third ventricle
- partial or complete absence of septum pellucidum.
Disorders of diverticulation
Septo-optic dysplasia:
- agenesis of septum pellucidum
- dilation of lateral ventricles with flattened roofs
- hypoplastic optic chiasm,
nerves,
and infundibulum
- dilation of chiasmatic and suprasellar cisterns
- expansion of optic recess of third ventricles
Holoprosencephaly:
- alobar,
representing no division of the cerebral hemispheres,
with a large,
horseshoe-shaped single ventricular cavity,
thin,
anteriorly placed cerebrum and fused thalami
- semilobar,
with normal formation of dural,
interhemispheric fissure and falx,
partially separated thalami,
the presence of a rudimentary third ventricle and a possible presence of the splenium of corpus callosum.
- lobar,
consisting in the fusion of frontal lobes,
hypoplastic frontal horns of the lateral ventricles,
interhemispheric fissure missing rostrally but with the presence of body and splenium of corpus callosum and a hypoplastic aspect of the falx.
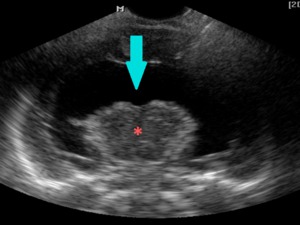
Fig. 16: Coronal section - Alobar holoprosencephaly - large, horseshoe-shaped single ventricular cavity (blue arrow) and fused thalami (pink star).
References: Department of Radiology, 3rd Pediatric Clinic, Cluj - Napoca
Aventricular cerebrum indicates the absence of the ventricles.
Disorders of sulcation
Lissencephaly:
- also known as smooth brain,
agyria or pachygyria
- failure of development of sulci and gyri
- increased depth of gray matter
- widened subarachnoid space
- minimal or no visible indentations
- Sylvian fissures shorter and more oblique
- absent pulsation of MCA in Sylvian groove
- mild-to-moderate ventricular dilation
- increased periventricular echogenicity
- no normal gray–white interdigitation.
Schizencephaly:
- clefts in brain,
often bilateral
- clefts lined by gray matter,
often along axis of normal fissure development.
- associated with ventricular dilation,
heterotopia,
polymicrogyria.
The disorders of size include microcephaly and macrocephaly,
which can be either familiar or associated with neurofibromatosis.
Hydrocehpalus may be an underlying cause of macrocephaly.
The destructive lesions which cause congenital anomalies of the brain include:
-hydranencephaly - in which the cerebral hemispheres are replaced by thin sacs of CSF,
with intact cranial vault,
meninges and falx
-porencephaly - representing an area of cavitation within the cerebral hemisphere caused by a periventricular hemorrhage,
a hypoxic-ischemic lesion,
infection,
trauma or surgery resulting in cystic structures
-hypoxia
-toxicosis
-inflammatory disease such as rubella,
cytomegalic inclusion disease,
toxoplasmosis and herpes simplex virus
Disorders of histiogenesis
- tuberous sclerosis - hereditary disorder characterized by epilepsy,
mental retardation and hamartomatous foci in the cerebrum,
cerebellum and spinal cord.

Fig. 17: Sagittal and coronal views - Tuberous sclerosis - marked echogenous intracerebral foci.
References: Department of Radiology, 3rd Pediatric Clinic, Cluj - Napoca
- neurofibromatosis - characterized by the presence of neurofibromas,
cutaneous pigmentary changes (many café-au-lait spots),
skeletal abnormalities, a predilection for certain tumors,
particularly within the central nervous system (optic pathway gliomas and astrocytomas),
vascular and endocrine abnormalities.
- Sturge–Weber syndrome (encephalotrigeminal angiomatosis)
- vascular lesions - Galen vein malformations,
arteriovenous malformations,
prediction of the risk for IVH and PVL,
evaluation of hydrocephalus - assessed with duplex and color Doppler,
transfontanellar and transcranial views.
Intracranial tumors:
- uncommon in children younger than two years
- supratentorial tumors are more common in infants
- neurologic criteria: macrocranium,
tumor erosion of the vault or clinical signs of increased intracranial pressure
- neuroectodermal origin
- teratoma is the most frequent type
- other tumors: glioma, astrocytoma,
lipma of the corpus callosum,
primitive neuroectodermal tumor,
choroid plexus papilloma,
ependymoma and ganglioglioma.
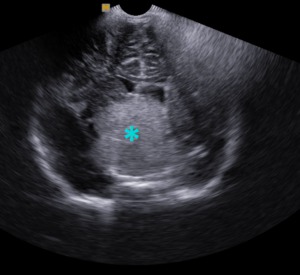
Fig. 18: Coronal section - Intracranial tumor (blue star - glioma).
References: Department of Radiology, 3rd Pediatric Clinic, Cluj - Napoca
Ultrasound is not able to differentiate between the various cell types,
but the size and location of the masses can give clues that can limit the differential diagnosis.
Intracranial teratomas:
- large echogenic lesions
- contain cystic spaces and echogenic areas with acoustic shadowing,
given by calcifications
- located mainly in the pineal region,
but also in the suprasellar and posterior fossae
- may obstruct the ventricular system or erode the skull
- uniformly fatal.
Gliomas:
- lesions in the brain stem
- hyperechoic compared with the cerebral hemispheres
- difficult to recognize in the normal hyperechoic cerebellum
Intracranial arachnoid cysts:
- the most common congenital cystic abnormality of the brain.
- fluid-filled cavities
- primary cyst caused by abnormal leptomeningeal formation or secondary caused by arachnoid adhesions
- may communicate with the subarachnoid space
- supratentorial or infratentorial
- most often located in the Sylvian fissure or temporal region.
- produce mass effect and hydrocephalus.
Intracranial infection
Common causative organisms for brain infections:
- group B streptococcus
- Escherichia coli
After the neonatal period:
- Haemophilus influenzae
- Streptococcus pneumoniae
- Neisseria meningitides
Ventriculitis is a common complication,
because of hte entrance of the organisms at the level of the choroid plexus.
Perinatal intracranial infections may also be secondary to viral or protozoan agents:
- cytomegalovirus (CMV)
- Toxoplasma gondii
- rubella
- herpes simplex virus type 2
Ultrasound findings:
Meningitis:
- increase in echogenity of the cortical sulci
- widening of the sulcal echoes
- small fluid collections
- ventricular enlargement in late stages
Ventriculitis:
- its presence increases mortality and morbidity.
- dilated ventricles,
with thickened,
irregular,
hyperechoic ependyma
- irregular,
hyperchoic choroid plexus
- intraventricular septations may develop
- better seen on US than on CT
- vasculitis and venous thrombosis may occur
Meningoencephalitis:
- increased parenchymal echogenity
- multiple,
patchy pattern
- increased gyral echogenity
- decreased vascular pulsations are noted.
- meningeal thickening - more than 1.3 mm over a gyrus or more than 2 mm over a sulcus
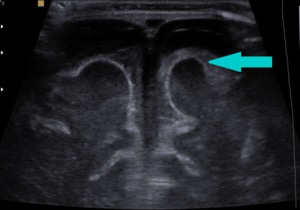
Fig. 19: Coronal section - increase in echogenity of the cortical sulci (blue arrow) in a case of meningitis.
References: Department of Radiology, 3rd Pediatric Clinic, Cluj - Napoca
Abscess:
- caused by Proteus mirabilis or Citrobacter diversus
- well-circumscribed lesion with a hypoechoic center,
fluid–debris level and thick,
echogenic wall
- may compress the ventricles or cause midline shift
Cytomegalovirus:
- gyral abnormalities: agyria, poly-microgyria,
focal microgyria,
calcification (usually periventricular),
hypoplastic cerebellum

Fig. 20: Coronal section - periventricular calcifications (white arrows) in a patient with CMV infection
References: Department of Radiology, 3rd Pediatric Clinic, Cluj - Napoca
Toxoplasmosis:
- calcification (periventricular and cortical),
- microcephaly
- hydrocephalus
- atrophy
- porencephaly
Herpes simplex virus:
- diffuse cerebral edema,
- diffuse cerebral atrophy
- multicystic encephalomalacia
- punctate or gyriform calcification
- cerebellar involvement
Rubella:
- areas of ischemic necrosis
- scattered calcifications (basal ganglia, white matter,
and periventricular)
- ventriculomegaly
Cephalohematoma:
- the most common injury of the skull in the newborn period
- appears after birth trauma as a soft-tissue lesion
- located mostly in the parietal and occipital regions
- bound by the sutures
- elliptical hypoechoic collection with areas of increased echogenity,
representing blood in different states
- does not cross the suture,
which can be observed with sonography.




. References: Department of Radiology, 3rd Pediatric Clinic, Cluj - Napoca")
. References: Department of Radiology, 3rd Pediatric Clinic, Cluj - Napoca")
. References: Department of Radiology, 3rd Pediatric Clinic, Cluj - Napoca")
. References: Department of Radiology, 3rd Pediatric Clinic, Cluj - Napoca")
 - cystic transformation. References: Department of Radiology, 3rd Pediatric Clinic, Cluj - Napoca")
. References: Department of Radiology, 3rd Pediatric Clinic, Cluj - Napoca")
. References: Department of Radiology, 3rd Pediatric Clinic, Cluj - Napoca")
. References: Department of Radiology, 3rd Pediatric Clinic, Cluj - Napoca")

, hypoplastic cerebellar hemispheres. References: Department of Radiology, 3rd Pediatric Clinic, Cluj - Napoca")
 and fused thalami (pink star). References: Department of Radiology, 3rd Pediatric Clinic, Cluj - Napoca")

. References: Department of Radiology, 3rd Pediatric Clinic, Cluj - Napoca")
 in a case of meningitis. References: Department of Radiology, 3rd Pediatric Clinic, Cluj - Napoca")
 in a patient with CMV infection References: Department of Radiology, 3rd Pediatric Clinic, Cluj - Napoca")