ECR 2014 / C-2026
Ultrasound assessment of most frequent shoulder disorders
This poster is published under an open license. Please read the disclaimer for further details.
Congress:
ECR 2014
Poster Number:
C-2026
Type:
Educational Exhibit
Keywords:
Trauma, Athletic injuries, Arthritides, Education, Diagnostic procedure, Ultrasound, Musculoskeletal soft tissue, Musculoskeletal joint
Authors:
S. P. Ivanoski; Ohrid/MK
DOI:
10.1594/ecr2014/C-2026

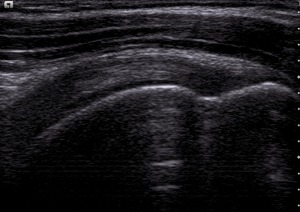
Fig. 1:
Normal supraspinatus tendon, longitudinal view

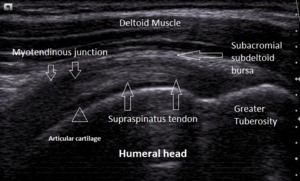
Fig. 2:
Supraspinatus tendon, normal anatomy, longitudinal view

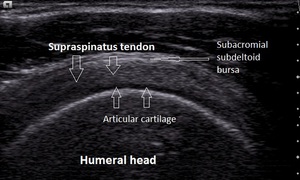
Fig. 3:
Supraspinatus tendon, transverse view

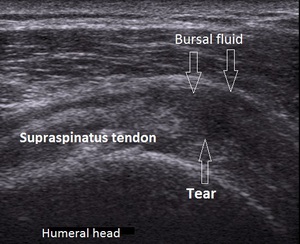
Fig. 4:
Supraspinatus tendon-bursal side partial thickness tear

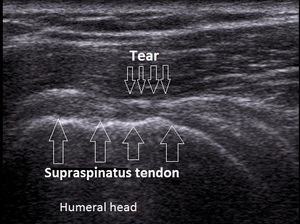
Fig. 5:
Supraspinatus tendon-full thickness chronic tear

Fig. 6:
Supraspinatus tendon tendinosis

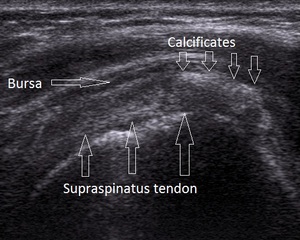
Fig. 7:
Supraspinatus tendon calcifying tendonitis

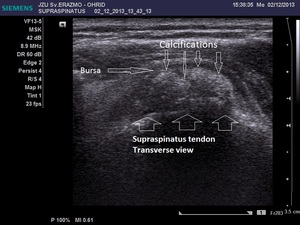
Fig. 8:
Supraspinatus tendon calcifying tendonitis-transverse view

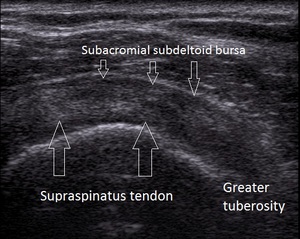
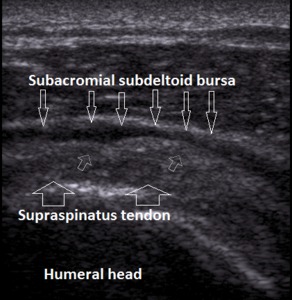
Fig. 9:
Subacromial subdeltoid bursitis

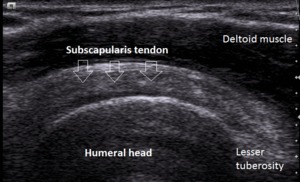
Fig. 10:
Normal Subscapularis tendon-longitudinal view

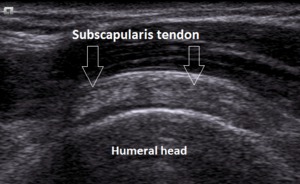
Fig. 11:
Normal subscapularis tendon-transverse view

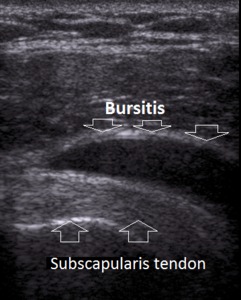
Fig. 12:
Subdeltoid bursitis

Fig. 13:
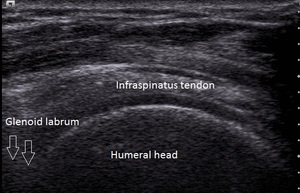
Normal Infraspinatus tendon-longitudinal view

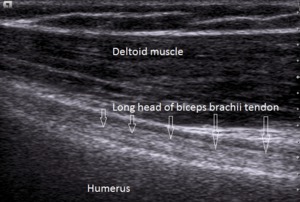
Fig. 14:
Tendon of long head of biceps brachii-longitudinal view

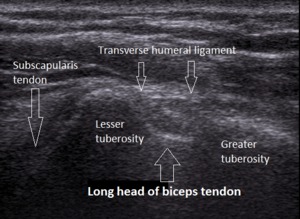
Fig. 15:
Tendon of long head of biceps brachii in the bicipital groove-transverse view

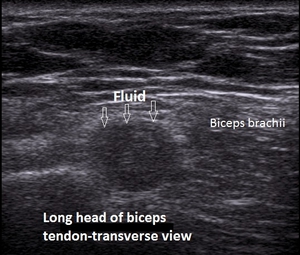
Fig. 16:
Degeneration of the tendon of long head of biceps brachii-transverse view

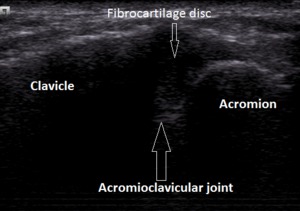
Fig. 17:
Acromioclavicular joint

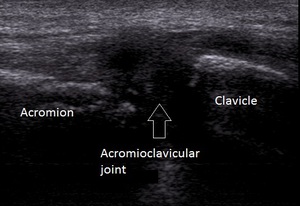
Fig. 18:
Acromioclavicular joint osteoarthritis