Plain imaging is the initial modality of choice for the workup of trauma in children in most Paediatric and General Accident and Emergency Departments. Adjunct ultrasonographic assessment is becoming more frequent. Nonetheless,
the safe interpretation of the child’s post trauma radiograph necessitates the understanding of the different mechanics of the immature skeleton.
Fractures in the growing bones of children are subject to influences that do not apply to adult bone [2]:
- Children’s bones are less brittle and more liable to plastic deformation – hence torus and greenstick fractures only occur in children.
- The periosteal sleeve is thicker than in adult bone and may explain why fracture displacement is more controlled.
- Cellular activity is also increased in the children – hence children’s fractures heal much more rapidly than those of adults.
- Bone growth involves both modeling and remodeling: this makes for a considerable capacity to reshape fracture deformities.
The term “buckle” fracture is an alternative term for a torus fracture but is sometimes,
rather imprecisely,
used to describe both greenstick and torus fractures.
By definition,
these 2 paediatric entities differ:
A greenstick fracture [3] results from an angulation force. A break occurs on the convex side of the bone whilst the opposite cortex remains intact ( Fig. 1 , Fig. 2 , Fig. 3 ) – secondary to the elastic properties of the child’s thick periosteum.

Fig. 1: The so-called greenstick fracture derives its name from the semblance this fracture in children has to the break that occurs in a green stick with one side bending and the outer convexity breaking (a). Radiograph demonstrates a greenstick fracture at fibular shaft (b).
References: (a) Muscat J (2014) (b) Department of Paediatric X-ray and Ultrasound, Royal Alexandra Children's Hospital, BSUH NHS Trust, Brighton, UK
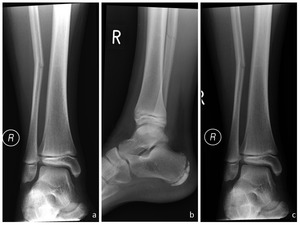
Fig. 2: Greenstick fracture of the fibula in an 11 year old boy who fell whilst playing football (frontal - a, lateral - b). Same fracture re-assessed 3 days later (c).
References: Department of Paediatric X-ray and Ultrasound, Royal Alexandra Children's Hospital, BSUH NHS Trust, Brighton, UK
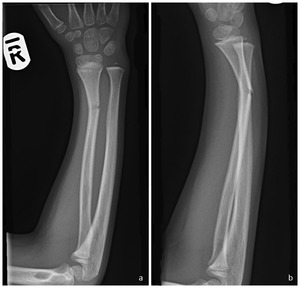
Fig. 3: Greenstick fracture of the distal radius in a 6 year old boy after a fall on the outstretched hand.
References: Department of Paediatric X-ray and Ultrasound, Royal Alexandra Children's Hospital, BSUH NHS Trust, Brighton, UK
A typical buckle (torus) fracture results from axial loading producing outward buckling of the cortex [1]. Hyperextension,
hyperflexion,
valgus or varus forces associated with axial loading produces an angled buckle fracture – presenting as angulation of the cortex [1,4]
( Fig. 4 ).

Fig. 4: A classic buckle (torus) fracture is the cortical bulging that occurs secondary to axial loading on the bone (a). When there are other forces associated with axial loading (in this case a valgus force) (b) , there is unilateral accentuation of the compression resulting in an angled buckle fracture(c).
References: Adapted from: Hernandez JA, Swischuk LE, Yngye DA, Carmichael KD. (2008) The angled buckle fracture in pediatrics: a frequently missed fracture. Emergency Radiology 10:71-75
When a longitudinal compressive force is insufficient to cause a greenstick fracture,
a plastic bowing fracture may occur in children. This type of fracture is caused by numerous “microfactures” along the convex border of the deformed bone secondary to axial loading of the bone. These microfractures are not visible on plain radiography [1].
Where to look?
- The distal radius is the commonest site involved ( Fig. 5 ).

Fig. 5: Torus fractures of the distal radius (a-f). Note the associated buckle fracture in the distal ulna in e and f.
References: Department of Paediatric X-ray and Ultrasound, Royal Alexandra Children's Hospital, BSUH NHS Trust, Brighton, UK
- The proximal radius is a common site for missed buckle fractures.
- Angled buckle fractures are easily missed: special attention has to be paid to the contour of the bone particularly at the metaphysis ( Fig. 6 ).

Fig. 6: Subtle dorsal angled buckle fracture and overlying soft tissue swelling demonstrated. Comparative views may be useful in cases such as this – but are not routine in our institution.
References: Department of Paediatric X-ray and Ultrasound, Royal Alexandra Children's Hospital, BSUH NHS Trust, Brighton, UK
- Angled buckle fractures are also common in the small bones of the hands ( Fig. 7 ) and feet (angled buckle fracture at base of the first metatarsal constitutes the “bunk-bed” fracture).
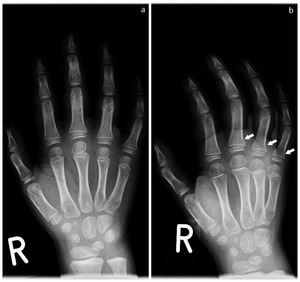
Fig. 7: Angled buckle fractures of the proximal 3rd, 4th and 5th metacarpals in a child with tenderness post trauma at this site.
References: Department of Paediatric X-ray and Ultrasound, Royal Alexandra Children's Hospital, BSUH NHS Trust, Brighton, UK
- Comparative views may be very useful in some cases.
- The presence of an elevated anterior fat pad may be the only indication of a fracture about the elbow.
In a child,
close inspection for a supracondylar fracture and an angled buckle fracture at the radial neck should ensue.
- Plastic bowing fractures ( Fig. 8 ) commonly involve the radius,
ulna,
clavicle and fibula. Again,
a high degree of suspicion is required.

Fig. 8: Plastic bowing fracture in a 4 year old who fell a height of just under 2m. Again, comparative views may be useful in clinching the diagnosis but are not routinely in use in our institution.
References: Department of Paediatric X-ray and Ultrasound, Royal Alexandra Children's Hospital, BSUH NHS Trust, Brighton, UK
Managing Buckle Fractures
Many authors have found buckle fractures to be inherently stable. Greenstick fractures are less stable – and have been found to continue to displace after 2 weeks [5] and hence the diagnosis of a greenstick fracture implies a more ‘severe’ injury – the latter demanding closer follow-up and more than the relatively simple splinting (back-slab) with or without specialist follow up required in a buckle fracture [5,6].

. Radiograph demonstrates a greenstick fracture at fibular shaft (b). References: (a) Muscat J (2014) (b) Department of Paediatric X-ray and Ultrasound, Royal Alexandra Children's Hospital, BSUH NHS Trust, Brighton, UK")
. Same fracture re-assessed 3 days later (c). References: Department of Paediatric X-ray and Ultrasound, Royal Alexandra Children's Hospital, BSUH NHS Trust, Brighton, UK")

 fracture is the cortical bulging that occurs secondary to axial loading on the bone (a). When there are other forces associated with axial loading (in this case a valgus force) (b) , there is unilateral accentuation of the compression resulting in an angled buckle fracture(c). References: Adapted from: Hernandez JA, Swischuk LE, Yngye DA, Carmichael KD. (2008) The angled buckle fracture in pediatrics: a frequently missed fracture. Emergency Radiology 10:71-75")
. Note the associated buckle fracture in the distal ulna in e and f. References: Department of Paediatric X-ray and Ultrasound, Royal Alexandra Children's Hospital, BSUH NHS Trust, Brighton, UK")


