ECR 2014 / C-2221
Understanding acute aortic syndrome: guide for a fast diagnosis and accurate reporting
This poster is published under an open license. Please read the disclaimer for further details.
Congress:
ECR 2014
Poster Number:
C-2221
Type:
Scientific Exhibit
Keywords:
Cardiovascular system, Vascular, CT-Angiography, CT, Echocardiography, Complications, Education, Structured reporting, Dissection, Acute, Blood
Authors:
M. C. Ageitos Casais, A. X. Martínez de Alegría Alonso, A. Arango, S. Baleato González; Santiago de Compostela/ES
DOI:
10.1594/ecr2014/C-2221

Fig. 2:
Aortic dissection: diagnostic findings

Fig. 3:
Aortic dissection: Diagnostic findings
- Intimal flap

Fig. 4:
Clues to identify the false lumen: larger lumen

Fig. 5:
Clues to identify false lumen:
- Delayed enhancement
- Surrounding true lumen

Fig. 6:
Clues to identify false lumen
- Thrombosed false lumen
- Beak sign

Fig. 7:
Aortic dissection: Differential diagnosis
- Mural thrombi

Fig. 8:
Aortic dissection: Complications
- Aortic rupture with pericardial effusion

Fig. 9:
Aortic dissection: complications
- Extension to supraortic trunk

Fig. 10:
Aortic dissection: complications
- Involvement of visceral arteries

Fig. 11:
Aortic dissection: complications
- Iliac arteries involvement

Fig. 12:
Intramural hematoma: unenhanced CT findings

Fig. 13:
Intramural hematoma: enhanced CT findings

Fig. 14:
Intramural hematoma: complications

Fig. 15:
Intramural hematoma: differential diagnosis

Fig. 16:
Penetrating atheromatous ulcer: pathogenesis

Fig. 17:
Penetrating atheromatous ulcer: ct findings

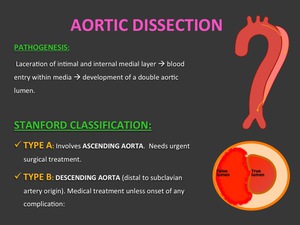
Fig. 1:
Aortic dissection: Pathogenesis and Stanford classification