ECR 2015 / C-0247
Autoimmune Pancreatitis – What every Radiologist needs to know now
This poster is published under an open license. Please read the disclaimer for further details.
Congress:
ECR 2015
Poster Number:
C-0247
Type:
Educational Exhibit
Keywords:
Pancreas, CT, Education, Cancer
Authors:
G. Miles, T. Adlan, F. Wotton, S. Jackson; Plymouth/UK
DOI:
10.1594/ecr2015/C-0247

Fig. 2:
Dr Henri Sarles - first described chronic pancreatitis with...
 Recent advances in autoimmune pancreatitis. Front Physio 3:374")
Fig. 3:
Clinical presentation/Histology/Treatment
 Chronic pancreatitis, pseudotumours and other tumour-like lesions. Modern Pathology 20:113-131")
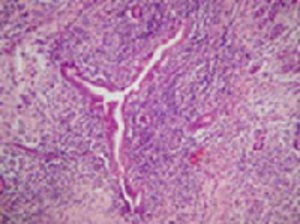
Fig. 4:
Type 1 AIP: Medium sized duct showing typical periductal lymphoplasmacytic...
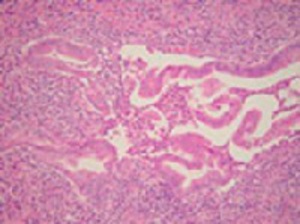
 - destruction of the epithelium by granulocytes References: Kloppel G. (2007) Chronic pancreatitis, pseudotumours and other tumour-like lesions. Modern Pathology 20:113-131")
Fig. 5:
Type 2 AIP: pancreatic duct showing a granulocytic epithelial lesion (GEL) -...

Fig. 6:
Various organs involved
 Chronic pancreatitis, pseudotumours and other tumour-like lesions. Modern Pathology 20:113-131")
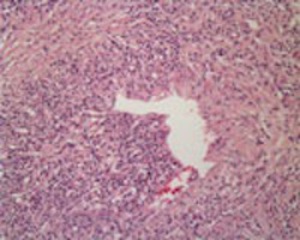
Fig. 7:
AIP: Obliterative venulitis

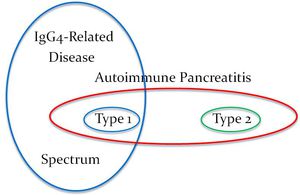
Fig. 8:
Schematic representation of AIP terminology
 Diagnosis & classification of autoimmune pancreatitis. J Auto Rev 13:451-58")
Fig. 9
 International consensus diagnostic criteria for AIP: guidelines of the International Association of Pancreatology. Pancreas 40(3):352-8")
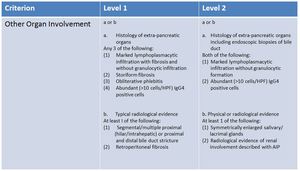
Fig. 10:
ICDC Original Guidelines of the International Association of Pancreatology
 International consensus diagnostic criteria for AIP: guidelines of the International Association of Pancreatology. Pancreas 40(3):352-8")
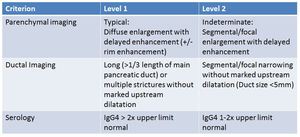
Fig. 11:
ICDC
 International consensus diagnostic criteria for AIP: guidelines of the International Association of Pancreatology. Pancreas 40(3):352-8")
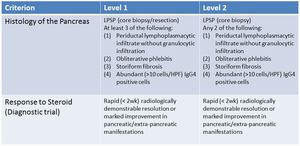
Fig. 12:
ICDC
 International consensus diagnostic criteria for AIP: guidelines of the International Association of Pancreatology. Pancreas 40(3):352-8")
Fig. 13:
ICDC
 International consensus diagnostic criteria for AIP: guidelines of the International Association of Pancreatology. Pancreas 40(3):352-8")
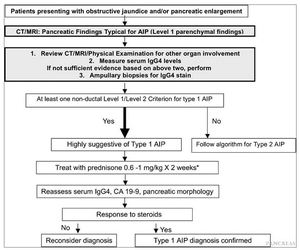
Fig. 14:
Type 1 AIP Diagnostic Algorithm
 International consensus diagnostic criteria for AIP: guidelines of the International Association of Pancreatology. Pancreas 40(3):352-8")
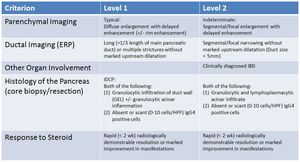
Fig. 15:
ICDC for Type 2 AIP