Imaging findings
I. Malignant endocervical glandular lesions showing gastric differentiation
1) Clinical features
GAS commonly affects middle aged women,
with age range from 37 to 84 years old,
with mean age of 42 years old [2; 3].
The typical presentation is vaginal bleeding or increased mucinous discharge. Although the clinical courses of GAS have not been extensively studied,
it is thought GAS is associated with aggressive behavior and a poor prognosis,
with propensity for peritoneal and adnexal involvement.
The patients commonly present with higher stage than the usual endocervical adenocarcinomas,
and this is considered to be resulting from delayed clinical diagnosis in many cases.
A 5-year disease-specific survival in GAS has been reported as 30%,
in contrast to that of 77% in usual endocervical adenocarcinoma [3].
Despite its extremely well differentiated appearance,
this worse prognosis also applied to MDA,
which have less favorable prognosis than the usual endocervical adenocarcinomas.
Only 20-30% of patients in any stage and 50% of stage I disease can survive beyond two years [9].
The poor prognosis in MDA may represent an exceptional example of clinical course in well-differentiated tumor.
2) Pathologic features
Macroscopically,
GAS and MDA typically present as an ill-defined and indurated infiltrating mass,
causing the swelling of the cervix,
which typically shows “barrel-shaped” appearance ( Fig. 2 ).
The mass may not be apparent at gross section,
since the tumor infiltrates into the cervical stroma while totally preserving the epithelium.
Microscopic appearance of GAS is characterized by the invasion of variably-sized epithelial glands into the cervical stroma.
The glands are irregularly-shaped and dilated,
and are composed of cells exhibiting characteristic features,
which are pale,
eosinophilic cytoplasm and distinct cell borders ( Fig. 1 ).
Immunohistochemically,
these glands are characterized by positivity for HIK1083 and MUC6,
which are the markers for gastric differentiation ( Fig. 2 ).
Another distinct feature of GAS including MDA and LEGH is an absence of high-risk HPV detection,
which can be monitored by the immunohistochemical marker of p16 [7; 8; 10].
It is widely assumed that the most of cervical adenocarcinomas are related to infection with high-risk human papillomavirus (HPV),
which is similar to squamous carcinomas.
The absence of HPV in cases of LEGH and GAS suggests that this sequence represents an HPV-independent pathway of carcinogenesis.
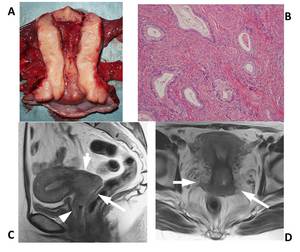
Fig. 2: Fig.2 Minimal deviation adenocarcinoma in a 40-year-old woman.
(A) Gross photograph of the uterus shows the swollen cervix without any epithelial mass. (B) Microphotograph of high power view shows diffusely infiltrating irregular-shaped glands composed of cells with eosinophilic cytoplasm. (C) Sagittal T2-weigthed image demonstrates an ill-defined cervical mass of slightly increased signal intensity (arrows). Note the tumor also extend into the anterior vaginal wall (arrowhead), though which is not visually apparent on the gross section. (D) Axial T2-weighted image demonstrate the infiltrating tumor in the cervix, also extending into the bilateral paramtrium.
References: Kyoto University Hostpital
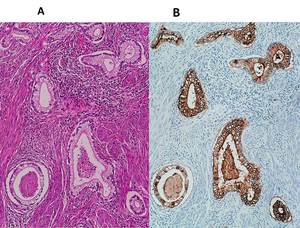
Fig. 1: Histopathology of minimal deviation adenocarcinoma, previously called adenoma malignum. (A) photomicrograph of low power view demonstrates irregular shaped glands in well-differentiated endocervical adenocarcinoma. (B) Immunochemical stain with HIK1083 demonstrates strong positivity in these neoplastic glands.
3) MRI features in correlation with pathologic features
MRI features of gastric type adenocarcinomas are characterized by the endophytic and infiltrative growth pattern into the cervical stroma without forming masses ( Fig. 2 ,
Fig. 3 ,
Fig. 4 ) [11].
The majority of the tumors are located in the upper portion of the cervix or in the entire cervix.
The tumors frequently invade into the corpus,
parametrium and vaginal wall ( Fig. 2 ).
This propensity for endophytic and infiltrating growth pattern may explain that patients of GMA commonly present with higher clinical stage.
The signal intensity of the tumors on T2-weighted images is variable,
ranging slightly increased high intensity to bright intensity ( Fig. 2 ,
Fig. 2 ,
Fig. 4 ).
This variable signal intensity may be considered to reflect histologic amount of mucin.
Another distinct characteristic in MRI finding of GAS is the presence of cysts of variable sizes in the tumors.
Some tumors may be associated with diffusely distributed irregular-shaped microcysts,
which are considered to represent neoplastic glands filled with mucin ( Fig. 3 ).
Some tumors may be accompanied by deeply located cysts of larger size,
which may represent preexisting benign endocervical glandular lesions such as LEGH ( Fig. 4 ).
However,
the presence of ill-defined and infiltrating mass can clearly indicate the malignancy.
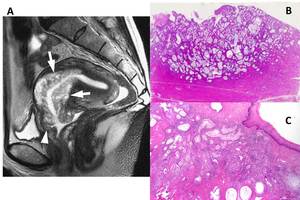
Fig. 3: Fig. 3Minimal deviation adenocarcinoma in a 47-year-old woman.
(A) Sagittal T2-weighted image demonstrates an ill-defined mass of heterogeneous high intensity, diffusely containing numerous irregular-shaped microcysts (arrows). The wall of the vaginal fornix is also thickened (arrowhaed), suggesting the involvement by the tumor. (B) Scanning magnification of the specimen shows the tumor composed of numerous dilated glands containing of mucin. (C) Microphotograph of the vaginal fornix shows infiltrating glands in the submucosal layer, totally preserving the surface epithelium.
References: Kyoto University Hostpital
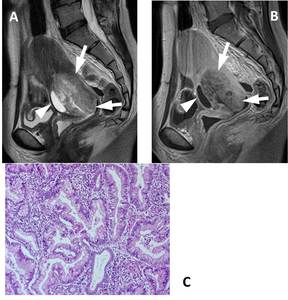
Fig. 4: Fig. 4 Gastric-type adenocarcinoma in a 43-year-old woman.
(A) Sagittal T2-weighted image and (B) post-contrast T1-weigthed image show an ill-defined mass causing the marked swelling the uterine cervix, exhibiting “barrel-shaped” appearance (arrows). The tumor contains irregular-shaped multiple microcysts. In the anterior portion of the cervix, there is a deeply located cyst (arrowhead), which may representing a part of pre-existing LEGH. (C) Photomicrograph of low power view shows invasive adenocarcinoma composed of irregular shaped glands showing gastric morphology.
References: Kyoto University Hostpital
These MRI findings are in contrast to the usual type of endocervical adenocarcinomas or much more common squamous cell carcinomas,
those typically exhibit exophytic growth from the cervical lip ( Fig. 5 ).
These tumors rarely associated with cysts.

Fig. 5: Fig. 5 Usual endocervical adenocarcinoma in a 36-year-old woman
Sagittal T2-weighted image demonstrates a mass of intermediate intensity (arrows), exhibiting exophytic growth from the anterior cervical lip.
References: Kyoto University Hostpital
4) The management of the patients
Historically,
MDA is notorious for its difficulty in establishing pathologic diagnosis.
The reasons in this difficulty may be attributed to lack of cytologic atypia in proliferating cells,
and the location of the upper cervix and endophytic nature of the growth pattern.
This difficulty in diagnosis on the biopsy may also be implicated in GAS.
Whenever the histologic evaluations failed in demonstrating malignancy in patients who presented with increased discharge,
repeated histologic evaluation and imaging studies including MRI should be recommended.
Once the pathologic diagnosis of GAS is established,
the management of the patients is determined according to the ordinary therapeutic strategy based on the clinical stage.
Although the implication of the radiation and chemotherapy remain investigated,
their efficacy may not be expected considering the poor prognosis in current status.
II. Benign endocervical glandular lesion showing gastric differentiation
1) Clinical features
LEGH commonly occur in middle aged women,
ranging from 37 to 71 year old (mean 45),
with similar age distribution to gastric-type adenocarcinomas.
The typical clinical manifestation is increased watery discharge.
However,
some patients may remain asymptomatic,
and LEGH may be incidental findings on imaging studies.
The incidence of LEGH was estimated as 0.7% in a review of consecutive hysterectomy and excision specimens.
The etiology of LEGH remains unknown,
but this condition is considered as a metaplastic process exhibiting gastric differentiation [10]and may be associated with chronic inflammation [12].
Rarely,
LEGH may be associated with Peutz-Jeghers syndrome (PJS).
2) Pathologic features
The gross appearance of LEGH is characterized by the multiple cystic space around the cervical canal,
and the lesion is typically located in the superior portion of cervix close to the internal os [5; 10].
LEGH is a well-demarcated lesion which is usually confined to the inner half of the cervix,
although occasionally there is extension into the outer half of the cervical wall [5].
Microscopic features in LEGH are characterized by the aggregates of small glands arranged in a lobular manner,
surrounding the ducts and the presence of deeply located cysts ( Fig. 6 ) [1].
The glands are lined by low columnar cells with pale eosinophilic cytoplasm and basally located small nuclei.
The most important differential diagnosis in LEGH is MDA.
The distinction made by the recognition of characteristic lobular arrangement of glands,
which contrasts with the haphazard arrangement of glands exhibiting heterogeneity in size and shape and focal areas of distinct nuclear atypia in MDA,
which often extends throughout the cervix ( Fig. 6 )[1].
However,
LEGH that exhibits a spectrum of architectural and/or cytologic abnormalities without evidence of stromal invasion are called as atypical LEGH.
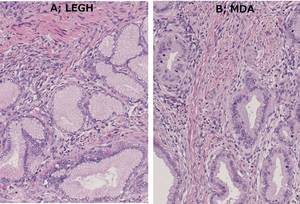
Fig. 6: Fig. 6 LEGH associated with MDA in a 74-year-old patient.
(A) Photomicrograph in an area of LEGH shows lobulated glands, lined by columnar cells with pale eosinophilic cytoplasm and basally located small nuclei. (B) photomicrograph of MDA shows tumor composed of haphazradous gland with some nuclear atypia, which lack lobular arrangement as seen in LEGH.
3) MRI features with pathologic correlation
The typical MRI features of LEGH are characterized by the aggregation of multiple small cysts of bright intensity on T2-weighted images,
surrounding the upper cervical canal nearby the internal os ( Fig. 7 ) [13-15].
The central portion of lesion consists of soft tissue of intermediate intensity,
corresponding to the proliferative endocervical glands,
which are the main pathologic nature of LEGH.
These features well correlates to the characteristics of the gross features described above.
The aggregated cysts are arranged in a floret-like manner,
which is known as “cosmos” (Cosmos bipinnatus) sign ( Fig. 7 )[1; 14].
These MRI features had previously been reported as those of adenoma malignum [16-19],
which is now known as MDA.
However,
this report was in the era before the entity of LEGH was described.
At that time,
LEGH might be easily confused as adenoma malignum,
since the histologic features differentiating these two entities have not been well established.
The photomicrographs in some of the papers reported as adenoma malignum may be considered to represent LEGH by the current criteria [1].
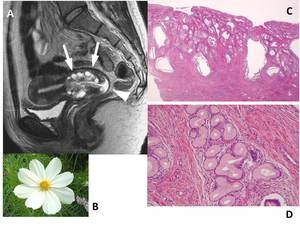
Fig. 7: Fig. 7 LEGH in a 35-year-old woman.
(A) Sagittal T2-weighted image sows the aggregation of multiple small cysts of bright intensity (arrows) like florets of cosmos, and the central soft tissue of intermediate intensity, surrounding the upper cervical canal. Note the presence of fluid in the vagina (arrowhead), representing the increased watery discharge in this patient. (B) Photograph of Cosmos bipinnatus. (C) Microphotograph of low power view showed deeply located cysts corresponding to the floret of cosmos and superficially situated endocervical glands which are essential histologic features of LEGH. (D) High power view shows loburated glands showing gastric glandular metaplasia.
References: Kyoto University Hostpital
Differential diagnoses for LEGH include Nabothian cysts and GAS.
In Nabothian cyst,
the number of cyst is limited,
and soft tissue along the cervical canal is virtually absent.
An important MRI finding for differentiating LEGH from GAS is the negative finding for an infiltrative mass beyond the deeply located cysts.
The aggregated cysts in floret-like manner (cosmos sign) may be absent in unusual case of LEGH,
in which differentiation from MDA may become difficult ( Fig. 8 ).
The preoperative MR diagnosis for atypical LEGH or LEGH associated with only microscopic GAS seems impossible ( Fig. 9 ).
The precise diagnosis of these conditions should rely on histologic findings of loop excision.

Fig. 8: Fig. 8; LEGH without cosmos sign in a 44-year-old woman.
Sagittal T2-weighted image shows a soft tissue mass along the cervcal canal and lip, without deeply located larger cysts. In this case, differentiation from MDA may be difficult.
References: Kyoto University Hostpital
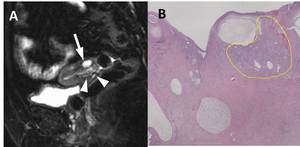
Fig. 9: Fig. 9; LEGH accompanied by microscopic foci of MDA in a 74-year-old patient (the same patient as Fig.6)
(A) T2-weighted image with fat suppression shows aggregated small cysts (arrowheads) accompanied by a deeply located cyst (arrow). (B) Photomicrograph of low power view shows an area of MDA composed of irregular-shaped glands (areas enclosed by dotted line), in the background of LEGH with multiple cysts.
4) The management of the patients
The suspicion of LEGH usually depends on imaging studies,
since LEGH is usually located at upper level of the cervix.
This is also why a biopsy oftne fails to yield the diagnosis of LEGH,
and loop excision may therefore be preferred for establishing the diagnosis.
Although LEGH was considered as a distinct benign condition since there was no recurrent disease in initial report,
subsequent report suggested that this conditions may occasionally be associated with invasive adenocarcinomas [7; 8].
Therefore,
when LEGH is suspected on imaging studies,
some gynecologists prefer hysterectomy to inquire whether there is coexisting adenocarcinoma or not.
However,
the implication of the surgery should be carefully determined,
especially when the fertility of the patient is an important issue.
Currently the exact risk of coexistence or future development of adenocarcinoma remains unknown,
although it is estimated to be low.
However,
in the presence of a clinically significant mass and/or massive watery vaginal discharge,
the patient should be managed with great caution [1].

 photomicrograph of low power view demonstrates irregular shaped glands in well-differentiated endocervical adenocarcinoma. (B) Immunochemical stain with HIK1083 demonstrates strong positivity in these neoplastic glands.")
 Gross photograph of the uterus shows the swollen cervix without any epithelial mass. (B) Microphotograph of high power view shows diffusely infiltrating irregular-shaped glands composed of cells with eosinophilic cytoplasm. (C) Sagittal T2-weigthed image demonstrates an ill-defined cervical mass of slightly increased signal intensity (arrows). Note the tumor also extend into the anterior vaginal wall (arrowhead), though which is not visually apparent on the gross section. (D) Axial T2-weighted image demonstrate the infiltrating tumor in the cervix, also extending into the bilateral paramtrium.
References: Kyoto University Hostpital")
 Sagittal T2-weighted image demonstrates an ill-defined mass of heterogeneous high intensity, diffusely containing numerous irregular-shaped microcysts (arrows). The wall of the vaginal fornix is also thickened (arrowhaed), suggesting the involvement by the tumor. (B) Scanning magnification of the specimen shows the tumor composed of numerous dilated glands containing of mucin. (C) Microphotograph of the vaginal fornix shows infiltrating glands in the submucosal layer, totally preserving the surface epithelium.
References: Kyoto University Hostpital")
 Sagittal T2-weighted image and (B) post-contrast T1-weigthed image show an ill-defined mass causing the marked swelling the uterine cervix, exhibiting “barrel-shaped” appearance (arrows). The tumor contains irregular-shaped multiple microcysts. In the anterior portion of the cervix, there is a deeply located cyst (arrowhead), which may representing a part of pre-existing LEGH. (C) Photomicrograph of low power view shows invasive adenocarcinoma composed of irregular shaped glands showing gastric morphology. References: Kyoto University Hostpital")
, exhibiting exophytic growth from the anterior cervical lip.
References: Kyoto University Hostpital")
 Photomicrograph in an area of LEGH shows lobulated glands, lined by columnar cells with pale eosinophilic cytoplasm and basally located small nuclei. (B) photomicrograph of MDA shows tumor composed of haphazradous gland with some nuclear atypia, which lack lobular arrangement as seen in LEGH.")
 Sagittal T2-weighted image sows the aggregation of multiple small cysts of bright intensity (arrows) like florets of cosmos, and the central soft tissue of intermediate intensity, surrounding the upper cervical canal. Note the presence of fluid in the vagina (arrowhead), representing the increased watery discharge in this patient. (B) Photograph of Cosmos bipinnatus. (C) Microphotograph of low power view showed deeply located cysts corresponding to the floret of cosmos and superficially situated endocervical glands which are essential histologic features of LEGH. (D) High power view shows loburated glands showing gastric glandular metaplasia. References: Kyoto University Hostpital")


(A) T2-weighted image with fat suppression shows aggregated small cysts (arrowheads) accompanied by a deeply located cyst (arrow). (B) Photomicrograph of low power view shows an area of MDA composed of irregular-shaped glands (areas enclosed by dotted line), in the background of LEGH with multiple cysts.")