1.
Diagnostic management
The diagnosis of breast cancer during pregnancy is more complicated due to the physiological changes occurring in breast during this period.
Ultrasound is the imaging modality of choice in evaluating breast abnormalities during pregnancy and lactation,
and therefore also in the diagnosis of breast cancer associated with pregnancy since it does not use ionizing radiation and has a high sensitivity (100 %).
It allows differentiation between normal tissue and mass,
and characterization of masses in the second case (benign or malignant characteristics).
However,
physiological changes also may alter the appearance of breast cancer and in some cases,
ultrasound features normally associated with benignity (parallel orientation,
posterior enhancement...) have been described in malignancies.
Aggressive neoplasms can disrupt blood supply leading to cystic degeneration or necrosis.
Therefore,
during pregnancy,
biopsy of any lesion that has no total criteria of simple cyst is recommended.
Ultrasound is also useful in detecting axillary lymphadenopathy and in monitoring the response to neoadjuvant chemotherapy.
In our review,
ultrasonography was performed as an initial test in all cases (11 patients).
In 7 patients the form of presentation was as an hypoechoic node-mass between 2'5-5cm,
perpendicularly orientated to the skin plane,
with ill-defined spiculated margins,
and occasionally with poor acoustic transmission.
In some of these 7 patients parallel orientation to the skin was observed,
however the rest of characteristics were highly suggestive of malignancy.
In 1 patient the nodule presented heterogeneous echogenicity and microlobulated contour.
In other 2 patients malignancies were presented as a complex mass with solid and cystic component,
paralel orientation to the skin,
and relatively well defined margins.
The solid pole showed heterogeneous echogenicity.
Finally,
in 1 patient was observed diffuse alteration of echogenicity,
poor planes differentiation,
and multiple nodules.
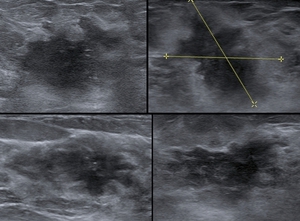
Fig. 1: Nodules of 4 different patients with malignancy features. All of them present an ill-defined contour, spiculated margin, altered echogenicity of the adjacent glandular tissue, some of them with perpendicular orientation to the plane of the skin, and one with
calcifications.
References: Department of Radiology. La Fe University and Polytechnic Hospital. Valencia/ES
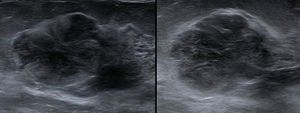
Fig. 2: 1 patient, solid nodule with heterogeneous echogenicity, parallel orientation to the skin, microlobulated contour.
References: Department of Radiology. La Fe University and Polytechnic Hospital. Valencia/ES
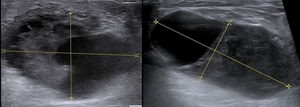
Fig. 3:
In 2 patients, nodules with mixed sonographic pattern with solid and cystic component.
References: Department of Radiology. La Fe University and Polytechnic Hospital. Valencia/ES
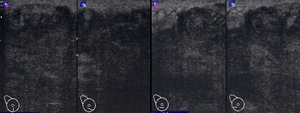
Fig. 4: Diffuse alteration of echogenicity, with multiple nodules. In righ picture, nodular image (marked with crosses)
References: Department of Radiology. La Fe University and Polytechnic Hospital. Valencia/ES
In summary,
although some nodules sometimes presented an isolated benign feature,
the rest of findings were highly suggestive of malignancy,
and lesions were classified in categories from BI-RADS4B to BI-RADS 5.
Physiological changes in the breast,
translates in mammography,
in variations of glandular density,
which adopts a dense and confluent appearance,
with decreased fat tissue.
Due to these changes there is a decreasing in the technique sensitivity.
Performing mammography is indicated in patients with clinical alteration to support the ultrasound findings,
since it identifies calcifications and could help in detecting bilateral or multicentric malignancies.
The realization of routine technique of mammography with two projections is possible during pregnancy using abdominal protection with low risk to the fetus.
The radiation received by the fetus would theoretically be 0'004Gy.
However,
general recommendations are avoiding mammography during the first trimester,
which covers the period of organogenesis,
when the fetus is more susceptible to radiation.
During lactation is recommended performing its realization immediately after emptying the breast,
in order to reduce breast density,
nevertheless its usefulness is limited.
The findings suspicious for malignancy are the same as in non-pregnant patients,
including mass/nodule,
microcalcifications,
asymmetrical density,
alteration of the structure and skin thickening or nipple retraction.
Mammography was performed in 7 of our 11 cases,
in 2 cases we don't have data about its realization,
and in the remaining 2 cases it was not performed because breast cancer diagnosis was made during the first trimester of pregnancy. In 4 patients only an asymmetry of breast density was observed,
in some cases it was very subtle,
and in the others it had nodular appearance.
In 1 patient a mass with features suggestive of benignity was observed,
and 1 patient presented an increased density,
trabecular reinforcement,
mass and skin thickening on affected quadrants.
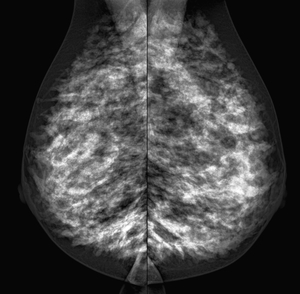
Fig. 5: Retroareolar left breast carcinoma. Only a minimal
asymmetry in the glandular density in retroareolar left breast localization is observed.
References: Department of Radiology. La Fe University and Polytechnic Hospital. Valencia/ES
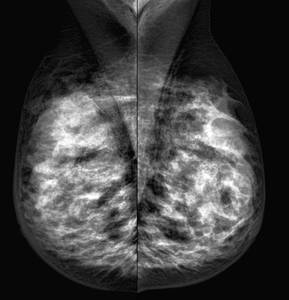
Fig. 6: Nodular asymmetry with ill-defined contour in upper quadrants of the right breast. Corresponds to a carcinoma in upper-outer quadrant of the right breast.
References: Department of Radiology. La Fe University and Polytechnic Hospital. Valencia/ES
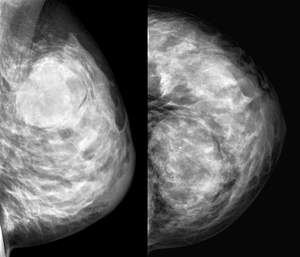
Fig. 7: In upper-outer quadrant of left breast, mass with features suggestive of benignity: Well circumscribed margins and oval contour, coarse calcification. It corresponded to a carcinoma.
References: Department of Radiology. La Fe University and Polytechnic Hospital. Valencia/ES
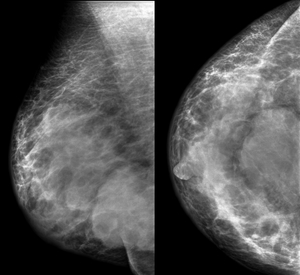
Fig. 8:
Mass with partially well circumscribed margins in the union between inner-lower and outer-lower quadrants. It associates a diffuse alteration of the density and skin thickening of right breast, predominant in lower quadrants and retroareolar localization, adjacent to the mass.
References: Department of Radiology. La Fe University and Polytechnic Hospital. Valencia/ES
In our patients,
as is refered in literature,
ultrasound proved more sensitivity and specificity in diagnosing and establishing the extent of lesions,
because physiological changes reduced the sensitivity of mammography in some patients.
The use of MRI during pregnancy in general terms is not accepted.
the safety of using contrast is not fully established and some studies have demonstrated its passage through the placenta and entry into fetal circulation.
Currently there is insufficient data on its potential impact.
Performing breast MRI during pregncy also presents technical difficulties since scanning is performed in prone position.
ACR only accepts the use of MRI on pregnant women in situations where the risk-benefit is clear and specifically notes that the contrast agents should not be used in this group of patients.
ESR states that the use of contrast is probably safe because the amount that is expected to cross the placental barrier is small and would be quickly eliminated by the fetal kidneys.
So far,
however,
the use of ultrasound and mammography is sufficient for the diagnosis of breast cancer during pregnancy.
MRI during lactation can be performed safely,
immediately after emptying the breast and leaving 24 hours for the next feeding,
since a minimum amount of contrast may be excreted by milk,
so this milk should be discarded.
The glandular parenchyma during lactation shows a rapid enhancement that can interfere with the detection of malignancies,
generating false positives,
though usually malignant nodules have higher and faster degree of enhancement than adjacent tissue.
MRI would have more usefulness in assessing the extent and multicentricity than in establishing the diagnosis.
In our patients MRI was only used in 3 cases.
In all the patients was performed to evaluate response to neoadjuvant chemotherapy,
before and after its administration.
In 2 of them was performed after voluntary interruption of pregnancy in first trimester and in 1 after cesarean during week 35 of pregnancy (neoplasm detected at week 32).
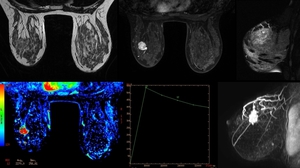
Fig. 10: MRI in a patient after VIP at week 5. Nodule in left breast, it shows microlobulated contour with early and intense enhancement, and subsequent washing. Features of high suspicion of malignancy.
References: Department of Radiology. La Fe University and Polytechnic Hospital. Valencia/ES
Establishing a definitive diagnosis requires an histological confirmation.
As
in non-pregnant women,
the sample for pathology study can be obtained safely by core needle biopsy guided by ultrasound under local anesthesia.
Although risk of milk fistula is described in literature,
its impact is minimal and it did not occur in any of our patients.
In cancer staging during pregnancy,
methods employing ionizing radiation should be avoided,
performing them if needed after the termination of pregnancy.
Some usual staging methods can be used safely during pregnancy.
These methods include chest radiograph with abdominal shielding,
liver ultrasound and total body MRI without contrast to evaluate column in case of suspicion of secondary bone involvement.
Metastases were observed in 3 of our cases.
2 of them had liver metastases at the moment of diagnosis and 1 developed pleural and bone metastases during the course of the disease.
Diagnosis of liver metastases was assessed by ultrasound and posteriorly was confirmed by CT.
Diagnosis of pleural and bone metastases was performed by CT and bone gammagraphy,
because they appeared during the course of the disease,
after completion of pregnancy.
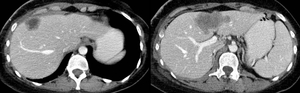
Fig. 12: Liver metastases in one patient. CT was performed after
pregnancy termination.
References: Department of Radiology. La Fe University and Polytechnic Hospital. Valencia/ES
2.
Descriptive analysis of clinical,
staging,
pathological features,
receptors,
and background risk
The usual presentation is like a painless palpable mass or nodule.
Physiological changes in breast imply an increase in breast density,
so palpation and therefore the detection of malignancies,
is hampered.
Other forms of presentation such nipple discharge are uncommon.
Regarding histology,
the most common is the invasive carcinoma of no special type (NST) (ductal NOS,
previously known as invasive ductal carcinoma),
being the other types less common.
Some of the studies suggest a lower proportion of positive hormone receptors and/or higher proportion of positiveness in Her2neu in gestational breast cancer,
while others do not.
In general,
there is no evidence of immunohistochemical and immunopathological differences from nonpregnant women for the same age group,
and it seems that the biological characteristics of the tumor may be more associated with age of the patient at diagnosis than associated to the gestational status.
In the literature it does not have been described specific risk factors associated with gestational breast cancer,
nor genetic,
nor environmental.
The incidence of BRCA1 or BRCA2 mutations neither has been higher than non-pregnant population.
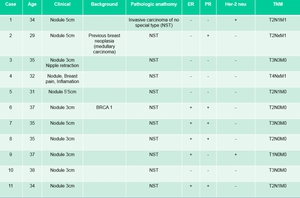
Fig. 13: Summary of clinical presentation, staging, pathological features, receptors, and background risk
References: Department of Radiology. La Fe University and Polytechnic Hospital. Valencia/ES
Our data are consistent with those described.
In all our patients clinical presentation of breast cancer was like palpable mass (between 3 - 6cm),
histology in all cases was grade 3 invasive carcinoma,
with hormonal receptors positiveness in 6 patients (54.5%),
negativeness in 5 patients (45.5%) and Her2-neu positiveness in 2 patients (18%).
Only relevant risk factors were found in 2 patients (18%),
one of them showed positive BRCA1 and the other one had a personal history of previous medullary breast carcinoma in both breasts.
In 3 patients metastases were observed (in 2 of them liver metastases at diagnosis and in 1 pleural and bone during the course of the disease). The age at diagnosis was between 29-38 years,
and most of the patients were older than 34 years old (70%).
3.
Cancer therapeutic management during pre- and postpartum,
pregnancy management,
and clinical evolution
The therapeutic options generally should be as similar as possible to the nonpregnant general population,
adapting them according to different characteristics in each case (gestational age at diagnosis,
stage,
receivers,
offspring wishes,
etc.) and considering fetal health.
Delay in diagnosis and treatment as well as prematurity should be avoided.
Also should be kept in mind that termination of pregnancy does not improve maternal prognosis.
There are many choices to consider in treating pregnant patients with breast neoplasia and they affect different specialties that must be coordinated between each other.
Therefore,
the therapeutic approach and management of pregnancy requires interdisciplinary collaboration,
and decisions must be agreed and taken from a multidisciplinary committee that comprise different specialties (medical and radiation oncology,
pathology,
radiology,
gynecology,
surgery...)
In general terms,
breast surgery can be performed during any trimester,
and election surgery should follow the same guidelines as for nonpregnant patients.
Selective sentinel node biopsy can also be used safely,
as the absorbed dose in the abdomen in nonpregnant patients is lower than the threshold of fetal dose (0'1Gy).
The use of radiotherapy is not approved during pregnancy,
however if conservative surgery is performed,
chemotherapy can be administrated and radiotherapy can be delayed after delivery.
As well as in surgery,
the decision to administer chemotherapy should also follow the same guidelines as in non-pregnant patients,
but should be administered after the first trimester,
as it covers the period of organogenesis.
Certain chemotherapy regimens have been accepted with safety for the fetus during the second and third trimester.
Other treatments such as monoclonal antibodies,
hormonotherapy or bisphosphonates can not be used during pregnancy because they are harmful to the fetus,
although its administration may be delayed after childbirth.
Certain supporting drugs commonly administrated during chemotherapy (granulocyte colony-stimulating factor,
certain types of corticosteroids) are not harmful to the fetus and could be used if needed.
Conventionally,
it has been argued that the prognosis in pregnant patients is worse compared to the general population,
however recent studies claim that it doesn't seems to exist worse prognosis compared to non-pregnant patients for the same age and stage.
So the worst prognosis is probably due to a later diagnosis at later stages because of breast physiological changes in pregnancy and lactation,
and/or because of the no standardization of treatment in this group of patients.
All our patients were followed in our hospital's multidisciplinary unit of breast pathology.
In all cases it was decided applying the standard treatment adjusting it individually to the special characteristics of each case,
as detailed in the table below.
We would like to remark that chemotherapy was used without fetal repercussions during the third trimester in some patients.
Two patients received a scheme of Anthracyclines + Cyclophosphamide,
reserving Taxanes to postpartum period due to lack of enough information about its fetal safety.
Another patient received chemotherapy in another hospital,
according to data available,
a scheme of Anthracyclines + Cyclophosphamide + 5-fluorouracil,
was administered.
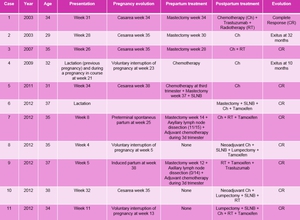
Fig. 14: Cancer therapeutic management during pre- and postpartum, pregnancy management, and clinical evolution
References: Department of Radiology. La Fe University and Polytechnic Hospital. Valencia/ES
Clinical evolution to the date has been similar to the non-pregnant population for the same age and cancer stage.
Two of the patients with metastatic disease evolved with progression despite treatment,
and resulted in death during the first 3 years after diagnosis,
and one of the patients evolved with a complete response,
remaining free of disease after 10 years (liver metastases).
With regard to pregnancy,
1 patient was diagnosed during breastfeeding and 3 patients decided voluntary interruption of pregnancy.
In the remaining 7 patients,
only in one case occurred a non-programmed preterm delivery at week 25 and in the other 6 patients,
delivery was scheduled between week 34-38 without any incidence.
All the fetuses were normal,
with no anomalies,
with normal weight to gestational age.
4.
Cases presentation
CASE 1
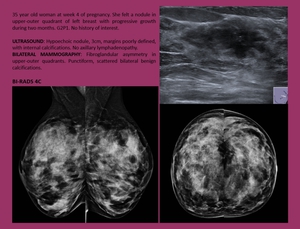
Fig. 15
References: Department of Radiology. La Fe University and Polytechnic Hospital. Valencia/ES
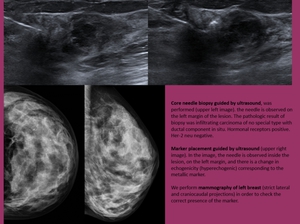
Fig. 16
References: Department of Radiology. La Fe University and Polytechnic Hospital. Valencia/ES
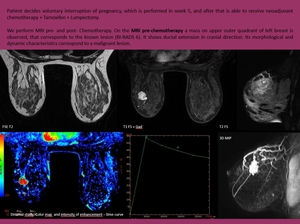
Fig. 17
References: Department of Radiology. La Fe University and Polytechnic Hospital. Valencia/ES
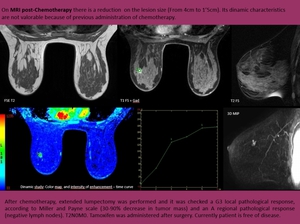
Fig. 18
References: Department of Radiology. La Fe University and Polytechnic Hospital. Valencia/ES
CASE 2
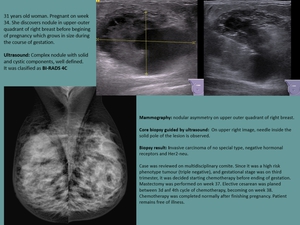
Fig. 19
References: Department of Radiology. La Fe University and Polytechnic Hospital. Valencia/ES
CASES 3 and 4
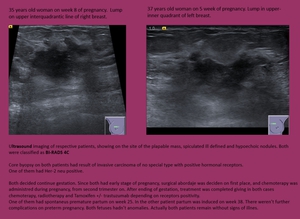
Fig. 20
References: Department of Radiology. La Fe University and Polytechnic Hospital. Valencia/ES
CASE 5
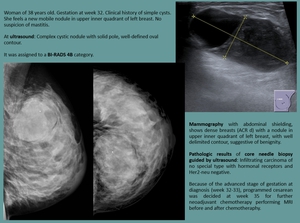
Fig. 21
References: Department of Radiology. La Fe University and Polytechnic Hospital. Valencia/ES
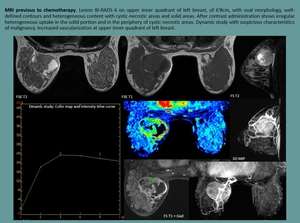
Fig. 22
References: Department of Radiology. La Fe University and Polytechnic Hospital. Valencia/ES




 References: Department of Radiology. La Fe University and Polytechnic Hospital. Valencia/ES")





. In the imagen of the left, the needle is observed in the left margin of the lession. In the second image, on the right, the presence of the needle is verified inside the lesion. References: Department of Radiology. La Fe University and Polytechnic Hospital. Valencia/ES")











