SKULL FRACTURES
- Bones are pliable in childhood,
so the fractures in pediatric patients are less common than adults.
-Types of calvarial fracture are linear,
depressed,
diastatic,
skull base,
ping pong and growing skull fracture (5).
- Linear skull fractures are the most common fractures.
Bones do not displace (Fig. 1).
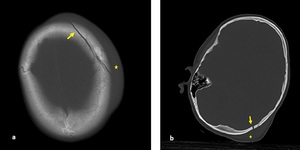
Fig. 1: Axial non-contrast enhanced CT (NECT) scan (a) and (b): a) A 7-year old boy was presented after a road trafic accident, nondeplaced fracture of left frontal bone (arrow) with soft tissue swelling (star). b) A 9-year old boy was presented after falling down from height, nondeplaced fracture of right occipital bone (arrow) with soft tissue swelling (star).
- Depressed skull fractures are the fragment of bone which is depressed deeper than the adjacent to inner table (Fig. 2).
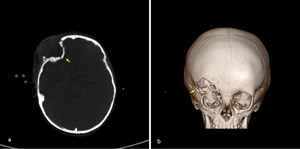
Fig. 2: Axial NECT scan(a) and CT 3D reconstruction (b): A 2-year-old girl was presented after a road traffic accident. (a-b) Depressed fracture of right inferior frontal bone (arrow).
- Diastatic skull fractures occur along the suture lines and usually affect newborns and infants in whom suture fusion has not yet happened.
In this type of fracture,
normal suture lines are widened.
- Skull base fractures locate in temporal bone or occipital condyl (Fig. 3). These fractures are often associated with dural tears,
which lead to rhinorrhea and otorrhea.
Temporal bone fractures are divided into 3 subtypes; longitudinal,
transverse and mixed type.
Longitudinal temporal bone fracture involves the squamous part of the temporal bone,
the superior wall of the external auditory canal,
and the tegmen tympani.
On CT,
a line parallel to the long axis of the petrous bone is seen.
The most common complications of longitudinal fractures are ossicular injury,
tympanic membrane rupture,
and hemotympanium.
Transverse temporal bone fracture is caused by trauma to the occipital or frontal regions or the craniocervical junction.
Fracture line is perpendicular to long axis of petrous bone.
Sensorineural hearing loss and fascial paralysis are commonly complications of transverse fracture.
Mixed fractures include both longitudinal and transverse fractures.
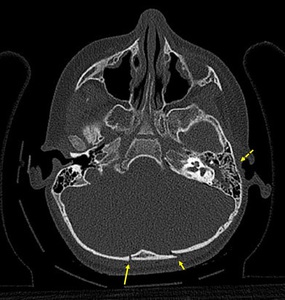
Fig. 3: Axial NECT scan: A 2-year old boy was presented after falling down from height. Bilateral occipital bone fractures which is nondeplaced on the right side (long arrow) and deplaced on the left side (short arrow), also, hemorrhagic opasification in left mastoid cells and middle ear cavity (dotted arrow). Temporal bone fractured could not be shown.
- Ping-pong skull fracture is likely a greenstick fracture of the long bones in children.
The fracture line appears concave (Fig. 4)
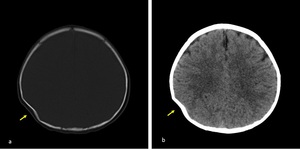
Fig. 4: Axial NECT scan with bone window (a) and parenchyma window (b): A 6-month old baby was presented after falling down from 2 meters. a) Ping pong fracture was seen in right parietal bone (arrow) b) parenchyme was normal.
- Growing skull fracture which occurs in younger than 3 years,
is a rare complication of head injury.
The lesion arises from a skull fracture with an associated dural tear and repeated pulsations of CSF.
Eventually,
the calvarial margin adjacent to fracture expands.
We can also use the term "leptomeningeal cyst" for this condition.
- In addition of these,
normal sutures,
accessory sutures and wormian bones imitate calvarial fractures.
Normal sutures and accessory sutures are usually bilateral and identified by their typical zigzag course and sclerotic borders.
On the other hand real fractures have linear fissur with lack of sclerotic margin (6).
Also,
swelling on the adjacent to soft tissue is an important finding which supports true fracture.
Moreover,
pneumocephalus and effusion in sinuses are indirect signs of bone injury (Fig. 5). Wormian bones are extra bone pieces that occur within a suture in the cranium.
Lambdoid suture is the most common location of wormian bones.
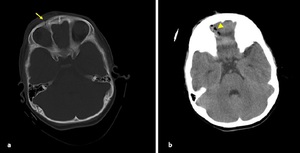
Fig. 5: Axial NECT bone window (a) and parenchyme window (b): A 2-year old girl was presented after falling down from 5 meters. a) Nondeplaced orbital floor fracture (arrow) b) pneumocephalus (arrowhead) was shown.
- It should not be forgotten that,
fracture line which is parallel to the section plane can be overlooked and it can be demonstrated by CT 3D bony reconstruction (Fig. 6).
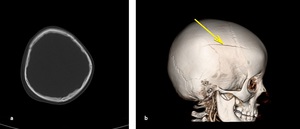
Fig. 6: Axial NECT scan (a) and CT 3D reconstruction (b): A 6-year old girl was presented after falling from 2 meters. a) Soft tissue swelling in right parietal region but fracture could not be seen. b) nondeplaced fracture of frontal and parietal bone was seen in CT 3D bony reconstruction.
EXTRAAXIAL HEMORRHAGE
Epidural hemorrhage (EDH)
- EDH occurs between the dura mater and calvarium.
- Caused by injury of the middle menigeal artery and its branches,
dural venous sinuses and veins.
- On CT it seems as hyperdense,
biconvex shaped collection in the extraaxial region.
It does not cross suture lines and can cross falx and tentorium (Fig. 7).
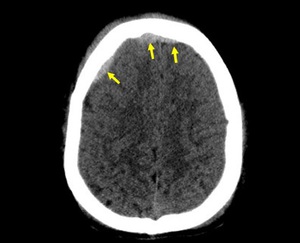
Fig. 7: Axial NECT scan: A 11-year old boy was presented after a road traffic accident. EDH was seen in right frontal region and crossed anterior falx (arrows).
- "Swirl sign" is hypodense area in hyperdense hemorrhagic collection,
that indicates actively bleeding (Fig. 8).
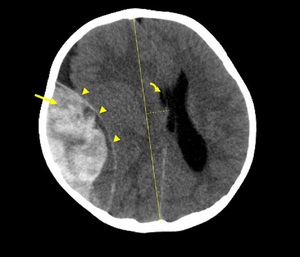
Fig. 8: Axial NECT scan: A 19-month old was presented after falling down from height. Large EDH was appeared lens like or biconvex shape in temporal location (arrowhead), heterogeneous appearance indicated active bleeding -swirl sign- (arrow), elevated intracranial pressure with absence of sulci, midline shift (dotted line) and compressed right ventricle (curved arrow).
- Calvarial fracture is generally associated with EDH.
- The most commonly region involved with EDH is temporal lobe in adults (temporal bone is relatively thin),
whereas this situation is rare in children.
Because the middle meningeal artery is closed to the inner table in adults but in children groove for middle menigeal artery has not formed yet.
Subdural hemorrhage (SDH)
- Located between the dura and arachnoid mater.
- Results from tearing of bridging veins.
- On CT it seems as hyperdense,
crescent-shaped collection in extraaxial region and may cross suture lines.
- Recurrent and mixed-age SDH should increase the suspicion of child abuse.
- Hyperacute SDH (± < 6 hrs); mostly hypodense (unclotted hemorrhage) on CT,
iso-hypointense on T1W-image and iso- hyperintense on T2W-image.
- Acute SDH (± 6 hrs-3 days); mostly homogenously hyperdense on CT (Fig. 9),
iso-hypointense on T1W-image and hypointense on T2W-image.
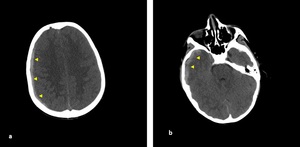
Fig. 9: Axial NECT scan (a-b): A 7-year old boy was presented after a road traffic accident. (a-b) acute SDH had a concave shaped in right frontoparietal and temporal lobes.
- Subacute SDH (± 3 days-3 weeks); iso- hypodense on CT.
Subacute SDH may have same density as underlying cortex and could be overlooked easily on CT.
Clues are medial displacement of gray and white matter junction,
increase in the distance between superficial brain parenchyma and adjacent to inner calvarial table,
displacement of enhancing cortical vessels. On T1W-image,
subacute SDH seems typically hyperintense and have variable intensity on T2W-image.
After iv gadolinium contrast injection; contrast enhancement may be seen.
- Chronic SDH (± > 3 wks); crescent-shaped and multiseptated extraaxial collection.
Calcification in 1-2%.
-Variable density depends on evolution of blood products.
After iv gadolinium contrast injected; enhancement surrounding membranes may be seen.
Subarachnoid hemorrhage (SAH)
- Occurs between the arachnoid and pia mater.
- SAH appears hyperdense on CT or hyperintense on FLAIR in basal cisterns,
sulci and Sylvian fissure (Fig. 30).
Intraventricular hemorrhage (IVH) develops via the Foramen Luschka and Magendie.
Typical appearence of IVH is blood-CSF level in occipital horns (Fig. 11).
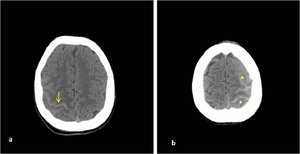
Fig. 10: Axial NECT scan (a-b) : a) A 16-year old boy was presented after a road traffic accident, SAH was hyperdense in sulcus of right parietal lobe. b) A 12- year old girl who fell from the height, SAH was seen in left frontal and parietal lobes.
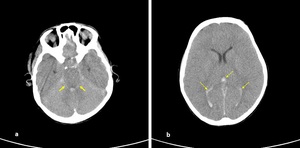
Fig. 11: Axial NECT scan (a-b): (a-b) A 12-year old girl was presented with a traffic accident. Hemorrhage in ambient cistern (arrow) and ventricular system (dotted arrow). Also, sulcal effacement and loss of differantiation between gray and white matter indicated brain edema.
- The complications of SAH are hydrocephalus,
infarction due to cerebral vasospasm and cerebral herniation,
so patients may rapidly progress to coma.
DIFFUSE AXONAL INJURY (DAI)
- Axonal damage occurs with axonal rotational acceleration and deceleration movement due to traumatic effect.
- DAI is also known as "shearing injury".
It is characterized by punctat hemorrhagic or nonhemorrhagic lesions.
- DAI locates in subcortical white matter (mild form),
corpus callosum (middle form) and brain stem (severe form).
- On CT initally often normal.
Small hypodense foci are seen in subcortical white matter,
corpus callosum or brain stem,
corresponding to edema of shearing injury. Punctate hemorrhagic lesions may appear as hyperdense foci on CT (Fig. 12).
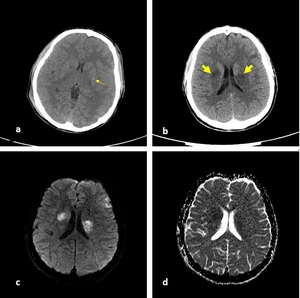
Fig. 12: Axial NECT scan (a-b) and b1000 DWI (c) and ADC map (d): A 15-year old boy was presented after a motorcycle accident. (a-b) hemorrhagic ( thinned arrow) and nonhemorrhagic (thickened arrow) DAI in basal ganglia. (c-d) restricted diffusion of nonhemorrhagic DAI was seen.
- MRI is more sensitive than CT to diagnose DAI.
If the children,
who have a normal initial CT scan,
get worse clinically; DAI should be considered and further evaluation with MRI should be done.
T2W- image shows multifocal hyperintense lesions at characteristic locations (Fig. 13). Especially,
SWI is the most sensitive imaging technique to detect hemorrhagic lesions.
Multifocal hypointense foci on SWI are seen due to susceptibility of blood products.
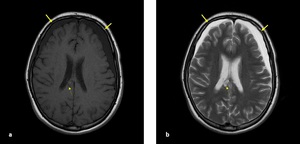
Fig. 13: Axial T1-W (a) and T2-W (b) images: A 15-year old girl was presented after a road traffic accident. (a-b) MRI was performed two months after the trauma, bilateral chronic SDH in frontal lobes (arrow) were seen hypointense on T1W,hyperintense on T2W and hemorrhagic DAI was seen in splenium of corpus callosum (dotted arrow).
CEREBRAL CONTUSION
- Characteristic location is adjacent to bony protuberance.
Anterior frontal lobe and temporal lobe are the most frequently affected regions from cerebral contusion (Fig. 14) (Fig. 15).
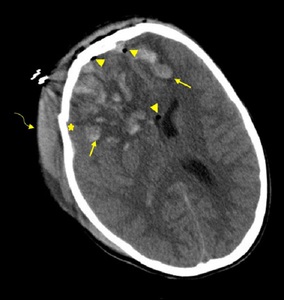
Fig. 14: Axial NECT scan: A 12-year old girl was presented after a road traffic accident. Contusion areas were seen in bilateral frontal lobes (arrows) with deplaced fracture of right frontal bone (star), soft tissue swelling (curved arrow) and pneumocephalus (arrowheads). Right lateral ventricle was compressed due to edema.
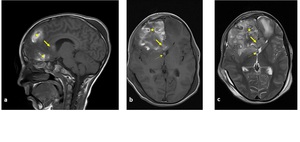
Fig. 15: Sagittal (a), axial (b) T1-W and axial T2-W images (c): (a-c) contusion areas were seen in frontal lobes (star), hyperintensity of genu of corpus callosum (arrow) and right side of fornix indicated hemorrhagic DAI (dotted arrow) in both images (same patient in "Fig. 14").
- Generally multifocal and bilaterally,
but focal contusion may also occur adjacent to depressed skull fracture.
- CT may be normal in the early phase or patchy,
ill-defined lesions may be seen as hyperdense foci (Fig. 16).
CT scan can be subtle due to Beam Hardening artefact.
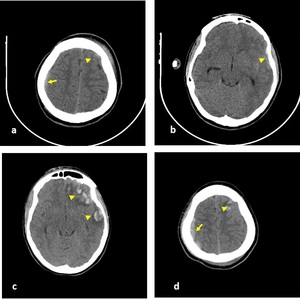
Fig. 16: Axial NECT scan (a-d): A 14-year old boy who had an epilepsy and was presented after falling down from height. (a-b) First CT image after admission, subtle EDH was seen in right frontoparietal lobe (arrow) and subtle hemorrhagic contusion areas were seen in left frontal lobe (arrowheads). (c-d) CT scan was performed after three days from admission, EDH and hemorrhagic contusion were revealed.
- MRI is the best imaging techique to detect hemorrhagic lesions (Fig. 17).
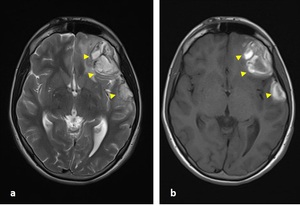
Fig. 17: Axial T2-W(a) and T1-W(b) images: (a-b) subacute contusion areas were seen hyperintense (arrowheads) in both images after 12 days from admission (same patient in "Fig. 16").
Especially,
SWI is the most sensitive imaging technique to detect hemorrhagic lesions (Fig. 18) (Fig. 19).
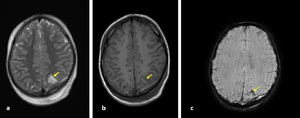
Fig. 18: Axial T1-W (a) and T2-W(b) images and Susceptibility-weighted image (c): A 9-year old boy was presented after falling down from 3 meters while he was on the bike. These images were performed 10 days after trauma. (a-b) subacute hemorrhagic contusion (arrow) was seen hyperintense in both sequences in left parietal lobe and (c) this area appeared hypointense due to susceptibility of blood products on SWI (curved arrow).
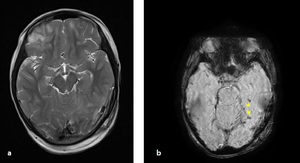
Fig. 19: Axial T2-W image(a) and SWI(b): microbleeding focuses were revealed on SWI in left temporal lobe (arrowheads), were not seen on conventional MRI sequences (same patient in "Fig. 18").
- "Coup" lesion; damage occurs at site of impact.
"Contrecoup" lesion; damage occurs at the opposite site of impact.
- Petechial hemorrhage may coalescence and become hematomas.
Herniation may occur due to mass effect of hematoma.
TRAUMATIC VASCULAR LESIONS
- Traumatic cerebrovascular injuries include minimal intimal injury,
dissection with intramural hematoma,
pseudoaneurysm,
occlusion,
transection with active hemorrhage and arteriovenous fistula (7).
They can cause ischemic stroke and are associated with high mortality rates.
- The most common mechanism of internal carotid artery injury is combined with hyperextension and contralateral rotation of the head and as a result; internal cartoid artery get streched nearby transverse process of C1 and C2 (7).
Furthermore,
bonny fragments caused by skull base or cervical spine fractures can injure the carotid or vertebral arteries.
- Cerebral angiography has a role in diagnosis and management of traumatic vascular injuries.
CT angiography (CTA) and MR angiography (MRA) are less invasive imaging techniques for detection of traumatic vascular lesions.
Internal carotid artery dissection with intramural hematoma
- Arteries have three layer: intima,
media,
adventitia.
- Dissection is a tear of tunica media.
Tearing leads to bleeding in the arterial wall.
- Hematoma occurs secondary to bleeding.
Absence of signal void ICA should be a sign of dissection on T1-W images.
Intimal flap can be seen in CTA or MRA.
Luminal diameter may vary according to presence of intramural hematoma (7).
Frequently,
narrowing of lumen,
which is described as a “string sign” is seen on angiography (8) (Fig. 20) (Fig. 21).
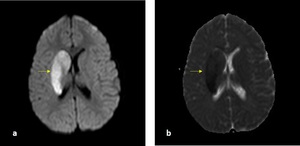
Fig. 20: b1000 DWI (a) and ADC map (b): A 6-year old girl was presented with left hemiplegia after falling from bicycle (a-b) acute infarct was seen in right basal ganglia (arrow).

Fig. 21: Coronal MIP(a-b) and axial 3D TOF image(c): Narrowing of lumen of right ICA and string sign (short arrows) indicated to ICA dissection (same patient in "Fig. 20").
Pseudoaneursym
- Pseudoaneursym is characterized by bubble formation from the native arterial wall.
It occasionally occur as a result of blunt trauma.
- Pseudoaneursym typically becomes symptomatic from 2-8 weeks after trauma.
- The most common complaint is pulsatile or nonpulsatile neck mass.
- On Doppler ultrasound,
lesions have a forward and backward flow,
so “to and fro” pattern with pulsed doppler may be seen and characteristic “yin-yang sign” may appear.
- On conventional MRI sequences; round or oval shaped lesion appears adjacent to the arterial wall.
If the lesion is thrombosed,
it can mimic a solid mass.
Transection with Active Hemorrhage
- Arterial transection is a laceration of all three layers of the vessel wall,
also known as arterial rupture.
- On CTA,
it appears as extravasation of contrast agent.
Arteriovenous Fistula (AVF)
- The abnormal communication between an artery and vein,
so early filling veins during arterial phase and enlarged drainage veins can be seen.
- A carotid cavernous fistula (CCF) is relatively more common than other traumatic AVF.
CCF is a communication between cavernous ICA and cavernous sinus.
On CTA or MRA,
it is seen as abnormal early filling of dilated cavernous sinus and dilated-tortuosed ipsilateral superior ophtalmic vein.
DIFFUSE CEREBRAL EDEMA
- Cerebral edeme is mainly divided into two categories; cytotoxic and vasogenic edema.
The ATP dependent Na/K pumps fails due to traumatic effect and cytotoxic edema is characterized by an increase in water content within the intracellular compartment in response to an osmotic gradient.
On the other hand,
vasogenic edeme occurs as a result of the blood-brain barrier disruption,
such as in intracranial hematoma secondary to head trauma,
brain tumours or infection.
Water moves from the vasculature to the extracellular space in response to an osmotic gradient (9).
- Imaging findings of diffuse cerebral edeme on CT; diffuse cerebral parenchymal hypoattenution and loss of normal differentiation gray and white matter,
effacement of sulci,
perimesencephalic and supracellar cistern,
compression of ventricular system (Fig. 22) (Fig. 23).
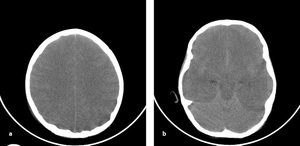
Fig. 22: Axial NECT scan (a-b): A 7-year old boy who was found while hanging on.a) Parenchimal low attenutation, effacement in sulci and loss of differentiation gray and white matter indicated to diffuse cerebral edema. b) cerebellar dansity increased in comparison with cerebral parenchyma -white cerebellum sign-.
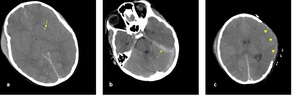
Fig. 23: Axial NECT scan (a,b,c): A 9-year old boy was presented after a road traffic accident. (a-b)hemorrhagic DAI was seen in left basal ganglia (arrow) and loss of differantion between gray and white matter, sulcal effacement and compression of lateral ventricles corresponded to diffuse cerebral edema. c) transcalvarial herniation (arrowheads) occured after the decompression craniectomy.
- White cerebellum sign: Cerebellum is relatively spared and appears hyperdense in comparison with hypodense cerebral parenchym.
- Pseudosubarachnoid hemorrhage: Dura and tentorium appear relatively hyperdense in comparison with hypodense cerebral parenchym.
TRAUMATIC HYPOXIC –ISCHEMIC BRAIN INJURY AND CORTICAL LAMINAR NECROSIS
- Hypoxic–ischemic brain injury occurs when mean arterial pressure falls below the lower limit of cerebral autoregulation.
- Thrombosis in the cerebral microcirculation occurs by the effects of trauma and contribute the evalution of secondary ischemic injury.
Intravascular thrombosis is seen more commonly in infants compare with older children and adults because of low flow states,
hemoconcentration and immature native antithrombotic pathways (10).
In addition,
the other cause of cerebral hypoxia is drowning in children.
The drowning results with arresting of alveolar oxygen exchange,
carbondioxide retension and vagally mediated cardiac arrest.
Consequently,
cerebral blood flow decreases.
So,
these entities result hypoxia and ischemia.
- Cortex and basal ganglia are highly metabolic active areas in brain.
They are the most vulnerable regions from effects of hypoxia.
- CT scan is usually be normal.
Loss of normal differentiation of gray and white matter,
hypodensity in deep gray matter and white cerebellum sign,
which is associated with cytotoxic cerebral edema,
indicate hypoxic-ischemic brain injury.
- Acute hypoxic abnormalities are difficult to detect in T1W and T2W sequences because of water content of brain and incomplete myelination especially in children under 2 years.
DWI is the most useful imaging technique in the diagnosis (10).
- DWI findings are restricted diffusion in vascular border zone areas and bilateral deep gray nuclei (Fig. 24).
Watershed infarctions occur at the border zones between major cerebral arterial territories as a result of hypoperfusion and they are seen more commonly in children than adults (10).
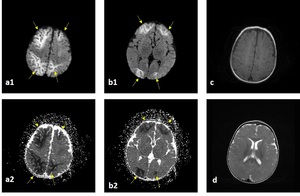
Fig. 24: b1000 DWI (a1-b1) and ADC map (a2-b2), axial T1-W (c) and axial T2-W (d) images: A 4-month old boy was presented after falling from 2 meters. (a-b) Diffusion was restricted symmetrically in bilateral anterior and posterior border zone areas. (c-d) T1-W and T2-W images were normal.
-Cortical laminar necrosis may be identified 2 weeks after trauma (peak period at 1 to 3 months).
Cortical linear hyperintensity indicates cortical laminar necrosis in T1-W image (Fig. 25)(Fig. 26).
An increased signal intensity on T1-W image is caused by the accumulation of denaturated proteins in dying cells.
Hemorrhage is not the reason of high signal.
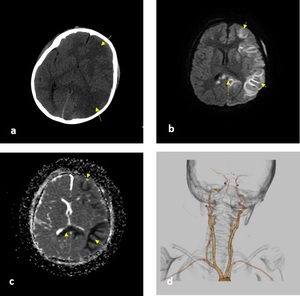
Fig. 25: Axial NECT (a), b1000 DWI (b) and ADC map (c) and CT 3D vascular reconstruction (d) : A 5-year old boy was presented after a road traffic accident and he had a loss of conciousness. A) low dansity areas in left frontal and parietooccipital lobes (long arrows) (b-c) restricted diffusion in cortical border zone areas of left cerebral hemisphere (short arrows) and genu of corpus callosum (dotted arrow) c) vascular structures were normal.
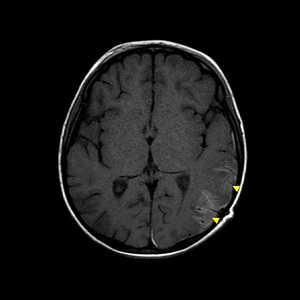
Fig. 26: Axial T1-W image showed that cortical linear hyperintensity (arrowheads) after 2 months from trauma (same patient in "Fig. 25")
- White matter lesions so-called “anoxic leukoencephalopathy” may occur in the late subacute or chronic phase.
- Cerebellum is relatively spared from effects of hypoxic ischemic brain damage.
Presence of cerebellar ischemia is a poor prognostic indicator.
LEPTOMENINGEAL CYST
- The other term is “growing skull fracture”.
- Rare complication of head injury.
- After the head trauma,
if the dura which is adjacent to the fractured bone tears,
the fracture is enlarged due to pulsation of CSF and leptomeningeal cyst may occur (Fig. 27).
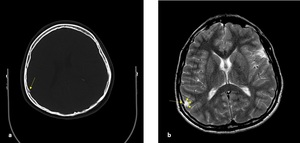
Fig. 27: Axial NECT scan (a) and axial T2-W image (b): A 8-year old boy was presented with a road traffic accident and these images were performed after 6 months from trauma a)fracture of internal tabula of right parietal bone (long arrow) b) small leptomeningeal cyst( short arrows) was adjacent to fracture of internal tabula.
- Parietal and temporal bones are most commonly involved bones.
- The most common fracture type leading to leptomeningal cyst is linear and diastatic,
and larger than 3-4mm (11).
- Differential diagnoses of leptomeningeal cyst are congenital (cephalocele) or iatrogenic (pseudomeningocele) cystic lesions.
Cephalocele is a brain herniation due to congenital calvarial fusion defects and pseudomeningocele is herniation of CSF or brain parenchyma after the postoperative bone defects (Fig. 28).
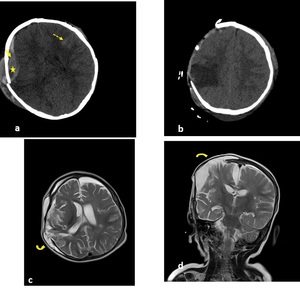
Fig. 28: Axial NECT scan (a-b) and axial (c) and coronal (d) T2W images: A 9-month old girl was presented after a road traffic accident. a) depressed fracture of right parietal bone, EDH (arrow) with swirl sign (star) and SAH in left frontal lobe (dotted arrow) b)she had a craniectomy operation (c-d) pseudomeningocele (curved arrow) was seen 3 weeks after the craniectomy operation.
HERNIATION
- Increasing of brain volume depends on hemorrhage or edema,
initially is compansated by displacement of CSF or blood.
When the mechanism is overpassed,
brain herniation may occur (Fig. 29).

Fig. 29: Six types of brain herniation 1) uncal 2) central transtentorial 3) subfalcine 4) extracranial 5) upward 6) tonsiller
- Uncal: Herniation of the medial temporal lobe downward from the tentorial incisura.
Uncal herniation may cause of Duret hemorrhages and midbrain ischemia because of compression to brainstem.
Duret hemorrhages are small linear hemorrhages along the midline of the brainstem and upper pons.
Also,
ipsilateral hemiparesia and third nerve palsy may occur (Kernohan's notch phenomenon).
- Central transtentorial: Herniation of the brainstem downward through the incisura.
IV.
cranial nerve palsy is an early finding of central herniation.
Occasionally,
posterior cerebral artery infarction can occur with central or uncal herniation.
- Subfalcine: Herniation of cingulate gyrus beneath the falx cerebri.
When the weakness of the contralateral lower extremity is determined,
the unilateral anterior cerebral artery compression should be thought.
- Extracranial: Brain tissue herniates through from the calvarial defect either iatrogenically or by trauma.
Sometimes it is termed as "fungus cerebri".
- Upward: Upward herniation is upward movement of the brain through the tentorium into the cranium.
- Tonsillar: Herniation of cerebellar tonsils downward into the foramen magnum.
Compression of the lower brainstem and medullary respiratory centers may result with sudden death.
CEREBROSPINAL FLUID (CSF) LEAKAGE
- Cerebrospinal fluid (CSF) leakage is movement of CSF from the intracranial cavity through an osseous defect within the skull base.
Disrupted dura and arachnoid mater is the cause of connection between intracranial cavity and nasal or middle ear cavity (12).
- Most common location of traumatic CSF leakage is the anterior cranial fossa.
Fracture of frontal sinus wall or cribriform plate present with rhinorrea.
- Temporal bone fractures which is through the mastoid cells or middle ear cavity present with otorrhea if the tympanic membrane is perforated.
- Clinical findings usually develop in the first 48 hours after injury,
and 95% manifest within the first 3 months.
A small subset of patients present with rhinorrhea or meningitis several years after the trauma.
- Undiagnosed CSF leak get complicated with meningitis or intracranial abscess.
- CT findings which increase suspicion of CSF leakage are pneumocephalus and an air-fluid level in sinuses.
In additionally,
asymmetrical opasification in mastoid cell and middle ear cavity,
fracture of tegmen tympani or inner ear structure may indicate CSF leakage (12).
- Diagnosing the fistula may be difficult.
In case of the suspicion of CSF leakage,
CT or MR cisternography should be used.
ENCEPHALOMALACIA AND ATROPHY
- Encephalomalacia and atrophy are parenchymal tissue loss with surrounding gliosis and dilatation of adjacent to ventricle.
They occur in the late period after the trauma.
- Focal tissue loss present as an encephalomalacia or porencephalic cyst.
Brain swelling,
increased intracranial pressure or hypoxia eventually cause diffuse parenchymal atrophy and tissue loss.
- Differantion between encephalomalacia and porencephalic cyst may sometimes be difficult.
Both entities show low density on CT.
Porencephalic cyst contains CSF and encephalomalacia has higher density than porencephalic cyst.
Porencephalic cyst has low signal intensity whereas encephalomalacia is seen hyperintense in FLAIR.
- Most common locations of encephalomalacia are anterior frontal and temporal lobes.
- Additionly,
severe head injury or diffuse white matter injury may cause the atrophy of corpus callosum.
Callosal atrophy indicates the disruption of interhemispheric connection and correlates with chronicity of injury.
Also,
loss of fornix and hypocampal volume may occur due to trauma.
CHILD ABUSE
- Nonaccidental injury is a leading cause of morbidity and mortality in infants and children.
- Infants have weaker neck muscles,
larger head compared with body and wider subarachnoid space than children and adults.
These are reasons of brain injury when infants are shaked.
- Different ages of subdural hematomas,
subarachnoid hemorrhage and retinal hemorrhage should increase suspicion of child abuse (13).


 scan (a) and (b): a) A 7-year old boy was presented after a road trafic accident, nondeplaced fracture of left frontal bone (arrow) with soft tissue swelling (star). b) A 9-year old boy was presented after falling down from height, nondeplaced fracture of right occipital bone (arrow) with soft tissue swelling (star).")
 and CT 3D reconstruction (b): A 2-year-old girl was presented after a road traffic accident. (a-b) Depressed fracture of right inferior frontal bone (arrow).")
 and deplaced on the left side (short arrow), also, hemorrhagic opasification in left mastoid cells and middle ear cavity (dotted arrow). Temporal bone fractured could not be shown.")
 and parenchyma window (b): A 6-month old baby was presented after falling down from 2 meters. a) Ping pong fracture was seen in right parietal bone (arrow) b) parenchyme was normal.")
 and parenchyme window (b): A 2-year old girl was presented after falling down from 5 meters. a) Nondeplaced orbital floor fracture (arrow) b) pneumocephalus (arrowhead) was shown.")
 and CT 3D reconstruction (b): A 6-year old girl was presented after falling from 2 meters. a) Soft tissue swelling in right parietal region but fracture could not be seen. b) nondeplaced fracture of frontal and parietal bone was seen in CT 3D bony reconstruction.")
.")
, heterogeneous appearance indicated active bleeding -swirl sign- (arrow), elevated intracranial pressure with absence of sulci, midline shift (dotted line) and compressed right ventricle (curved arrow).")
: A 7-year old boy was presented after a road traffic accident. (a-b) acute SDH had a concave shaped in right frontoparietal and temporal lobes.")
 : a) A 16-year old boy was presented after a road traffic accident, SAH was hyperdense in sulcus of right parietal lobe. b) A 12- year old girl who fell from the height, SAH was seen in left frontal and parietal lobes.")
: (a-b) A 12-year old girl was presented with a traffic accident. Hemorrhage in ambient cistern (arrow) and ventricular system (dotted arrow). Also, sulcal effacement and loss of differantiation between gray and white matter indicated brain edema.")
 and b1000 DWI (c) and ADC map (d): A 15-year old boy was presented after a motorcycle accident. (a-b) hemorrhagic ( thinned arrow) and nonhemorrhagic (thickened arrow) DAI in basal ganglia. (c-d) restricted diffusion of nonhemorrhagic DAI was seen.")
 and T2-W (b) images: A 15-year old girl was presented after a road traffic accident. (a-b) MRI was performed two months after the trauma, bilateral chronic SDH in frontal lobes (arrow) were seen hypointense on T1W,hyperintense on T2W and hemorrhagic DAI was seen in splenium of corpus callosum (dotted arrow).")
 with deplaced fracture of right frontal bone (star), soft tissue swelling (curved arrow) and pneumocephalus (arrowheads). Right lateral ventricle was compressed due to edema.")
, axial (b) T1-W and axial T2-W images (c): (a-c) contusion areas were seen in frontal lobes (star), hyperintensity of genu of corpus callosum (arrow) and right side of fornix indicated hemorrhagic DAI (dotted arrow) in both images (same patient in "Fig. 14").")
: A 14-year old boy who had an epilepsy and was presented after falling down from height. (a-b) First CT image after admission, subtle EDH was seen in right frontoparietal lobe (arrow) and subtle hemorrhagic contusion areas were seen in left frontal lobe (arrowheads). (c-d) CT scan was performed after three days from admission, EDH and hemorrhagic contusion were revealed.")
 and T1-W(b) images: (a-b) subacute contusion areas were seen hyperintense (arrowheads) in both images after 12 days from admission (same patient in "Fig. 16").")
 and T2-W(b) images and Susceptibility-weighted image (c): A 9-year old boy was presented after falling down from 3 meters while he was on the bike. These images were performed 10 days after trauma. (a-b) subacute hemorrhagic contusion (arrow) was seen hyperintense in both sequences in left parietal lobe and (c) this area appeared hypointense due to susceptibility of blood products on SWI (curved arrow).")
 and SWI(b): microbleeding focuses were revealed on SWI in left temporal lobe (arrowheads), were not seen on conventional MRI sequences (same patient in "Fig. 18").")
 and ADC map (b): A 6-year old girl was presented with left hemiplegia after falling from bicycle (a-b) acute infarct was seen in right basal ganglia (arrow).")
 and axial 3D TOF image(c): Narrowing of lumen of right ICA and string sign (short arrows) indicated to ICA dissection (same patient in "Fig. 20").")
: A 7-year old boy who was found while hanging on.a) Parenchimal low attenutation, effacement in sulci and loss of differentiation gray and white matter indicated to diffuse cerebral edema. b) cerebellar dansity increased in comparison with cerebral parenchyma -white cerebellum sign-.")
: A 9-year old boy was presented after a road traffic accident. (a-b)hemorrhagic DAI was seen in left basal ganglia (arrow) and loss of differantion between gray and white matter, sulcal effacement and compression of lateral ventricles corresponded to diffuse cerebral edema. c) transcalvarial herniation (arrowheads) occured after the decompression craniectomy.")
 and ADC map (a2-b2), axial T1-W (c) and axial T2-W (d) images: A 4-month old boy was presented after falling from 2 meters. (a-b) Diffusion was restricted symmetrically in bilateral anterior and posterior border zone areas. (c-d) T1-W and T2-W images were normal.")
, b1000 DWI (b) and ADC map (c) and CT 3D vascular reconstruction (d) : A 5-year old boy was presented after a road traffic accident and he had a loss of conciousness. A) low dansity areas in left frontal and parietooccipital lobes (long arrows) (b-c) restricted diffusion in cortical border zone areas of left cerebral hemisphere (short arrows) and genu of corpus callosum (dotted arrow) c) vascular structures were normal.")
 after 2 months from trauma (same patient in "Fig. 25")")
 and axial T2-W image (b): A 8-year old boy was presented with a road traffic accident and these images were performed after 6 months from trauma a)fracture of internal tabula of right parietal bone (long arrow) b) small leptomeningeal cyst( short arrows) was adjacent to fracture of internal tabula.")
 and axial (c) and coronal (d) T2W images: A 9-month old girl was presented after a road traffic accident. a) depressed fracture of right parietal bone, EDH (arrow) with swirl sign (star) and SAH in left frontal lobe (dotted arrow) b)she had a craniectomy operation (c-d) pseudomeningocele (curved arrow) was seen 3 weeks after the craniectomy operation.")
 uncal 2) central transtentorial 3) subfalcine 4) extracranial 5) upward 6) tonsiller")