ECR 2016 / C-1648
Scapular Dyskinesis: The role of MR Imaging.
This poster is published under an open license. Please read the disclaimer for further details.
Congress:
ECR 2016
Poster Number:
C-1648
Type:
Educational Exhibit
Keywords:
Musculoskeletal system, Musculoskeletal bone, Musculoskeletal soft tissue, MR, Education, Motility
Authors:
E. Camuera1, L. Fernandez Rodriguez2, I. Hafeez 3, R. Sharma3, J. Gómez4, J. M. Marin5, J. Beltran3; 1Bilbao/ES, 2Madrid/ES, 3Brooklyn, NY/US, 4León/ES, 5Leganés Madrid/ES
DOI:
10.1594/ecr2016/C-1648

Fig. 7:
Scapular dyskinesis types.
: 1–11")
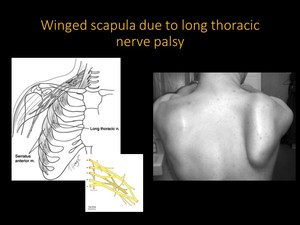
Fig. 8:
Winged scapula due to long thoracic nerve palsy. The long thoracic nerve passes...
: 1–11")
Fig. 9:
Scapular stabilizing innervation.
: 1–11")
Fig. 10:
Neurogenic causes of scapular winging.
, suggestive of chronic denervation changes due to long thoracic nerve palsy. References: Courtesy of Dr. Beltrán. Department of Radiology, Maimonides Medical Center. Brooklyn")
Fig. 11:
MRI of young female who practices archery. Axial T1 and STIR images show...

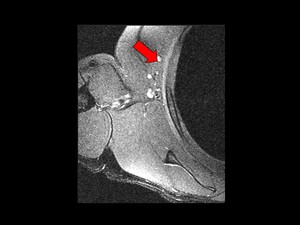
Fig. 12:
Axial STIR image reveals high intensity of the serratus anterior muscle. This...
 Axial and sagittal T1 MR images demostrate a high intensity mass in serratus anterior muscle indicative of elastofibroma dorsi with fat infiltration. c and d) Axial and sagittal STIR images show hyperintense elastofibroma dorsi and diffuse high intensity in serratus anterior muscle, sugestive of early denervation changes. References: Courtesy of Dr. Beltrán. Department of Radiology, Maimonides Medical Center. Brooklyn")
Fig. 14:
Patient with right elastofibroma dorsi located deep to serratus anterior...
 and the normal infraspinatus muscle (asterisk). References: G. Tsivgoulis Differential diagnosis of scapular winging Neurology 2012;78;e109")
Fig. 15:
A-C: Right scapular winging caused by weakness of ipsilateral trapezius. Arrow...

Fig. 13:
Glenohumeral pathologies graphic.
 Oblique sagittal T2 - MR show increased signal within the enlarged biceps tendon (white solid arrow) indicative of biceps tendinopathy. b) Axial PD-FS MR shows increased signal within the biceps tendon. c) Coronal oblique T2-FS MR shows full thickness rotator cuff tear. d) Sagittal T1 MR shows a type III acromion compressing the subacromial bursa and indenting the supraspinatus tendon (rotator cuff impingement). References: Diagnostic Imaging Muskuloskeletal. STATdx.")
Fig. 16:
Scapular dyskinesis associated pathologies.These impairments can be diagnose by...
Coronal oblique T2-FS MR shows a thickening and high signal of the axillary recess capsule and synovium,suggestive of adhesive capsulitis. b)Axial MR arthrogram T1-FS shows the tear involving the anterior (white solid arrow) and posterior labrum (white curved arrow), SLAP lesion. c) Axial PD-FS MR of a Bankart lesion. d) Axial T1 image shows Hill-Sachs lesion. References: Diagnostic Imaging Muskuloskeletal. STATdx.")
Fig. 17:
Another associated pathologies. a)Coronal oblique T2-FS MR shows a thickening...