ECR 2016 / C-1796
Treatment of emphysema: procedure planning and follow-up by HRCT
This poster is published under an open license. Please read the disclaimer for further details.
Congress:
ECR 2016
Poster Number:
C-1796
Type:
Educational Exhibit
Keywords:
Transplantation, Education and training, Chronic obstructive airways disease, Treatment effects, Surgery, Education, CT-Quantitative, CT-High Resolution, CT, Thorax, Lung, Interventional non-vascular
Authors:
G. Milanese1, M. Silva1, A. Borghesi2, M. Bezzi3, M. Bonifazi4, M. Novali2, N. Sverzellati1; 1Parma/IT, 2Brescia/IT, 3Firenze/IT, 4Ancona/IT
DOI:
10.1594/ecr2016/C-1796
. The evaluation of fissures and other parenchymal anomalies, namely bronchiectasis or bullae, is mandatory to guide the treatment decision. Notably, fissure integrity reflects absence of major collateral ventilation and is a necessary selection criteria for EBV positioning. Conversely, fissural defects (>10% on axial plane) and a residual amount of healthy tissue can be treated by LVRCs.")
Fig. 1:
Pattern of emphysema: the quantitative evaluation of emphysema by dedicated...
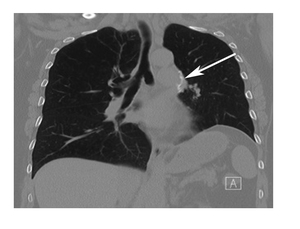
: coronal chest CT after LVRS shows increased opacity in the left hilum with metallic staple lines (white arrow) that are usually positioned during the surgical procedure. These are normal findings that should not be misdiagnosed as complications. References: Anand Devaraj, Royal Brompton Hospital, London, UK")
Fig. 2:
Post operative finding after lung volume reduction surgery (LVRS): coronal...
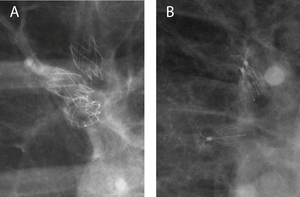
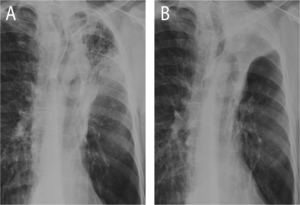
 currently available for treatment as for Conformitè Européenne (CE) qualification: (A) magnification of a chest X-ray in a patient treated with the duckbill EBV (Zephyr; Pulmonx, Inc., Palo Alto, CA, USA). (B) Magnification of a chest X-ray in a patient treated with the umbrella-shaped intrabronchial valve (Spiration; Olympus Respiratory America, Redmond, WA, USA).")
Fig. 3:
Radiographic evaluation after positioning of endobronchial valves (EBV)...
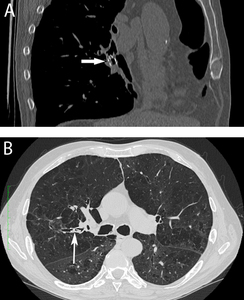
 multiplanar reformatted image (A) of oblique sagittal plane, in a patient treated with endobronchial valve (Zephyr; Pulmonx, Inc., Palo Alto, CA, USA), visible as a metallic structure in the bronchus lumen (white arrow). Axial chest CT with lung window reconstruction (B) after valve positioning in posterior segmental bronchus of the right upper lobe (Spiration; Olympus Respiratory America, Redmond, WA, USA). The valve is detectable as high-density linear structure within the bronchial lumen (white arrow).")
Fig. 4:
Endobronchial valves: computed tomography (CT) multiplanar reformatted image...
. Follow up after 5 weeks show progression of consolidation towards sharply demarked opacification reflecting atelectasis (B), a sign of successful treatment after EBV positioning.")
Fig. 5:
Atelectasis after endobronchial valve treatment: chest X-ray 1 day after valve...
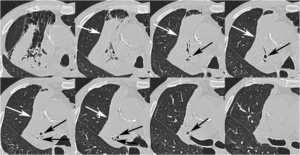
 show volume reduction of the right upper lobe.")
Fig. 6:
Atelectasis after endobronchial valve treatment: axial chest CT scans after...

Fig. 7:
Pattern of emphysema: volume rendering reconstruction of volumetric CT shows...

Fig. 8:
Infectious consolidation after endobronchial valve positioning: axial chest CT...
 reconstruction on the axial plane of a patient with severe emphysema treated with endobronchial valves in the right upper lobe. The reconstruction highlights the complex structure of the valves. The consolidation distal to the valves shows irregular margins and peribronchial distribution, which reflect infectious pneumonia rather than atelectasis.")
Fig. 9:
Consolidation after endobronchial valve positioning: maximum intensity...
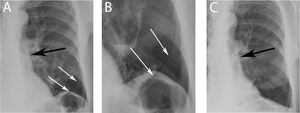
 and its magnification (B) show hyperlucency in the left costo-phrenic sulcus (white arrows) after EBV positioning (black arrow), reflecting pneumothorax (prevalence 6% after treatment by EBV). Resolution of pneumothorax is documented by chest X-ray follow-up (C).")
Fig. 10:
Pneumothorax after EBV: chest X-ray (A) and its magnification (B) show...
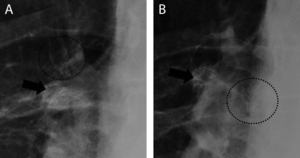
 performed during the follow-up after EBV positioning in the apical and anterior segmental bronchi of the right upper lobe. (B) The valve previously deployed in the apical bronchus has migrated into the right main bronchus.")
Fig. 11:
Migration of an endobronchial valve: chest X-ray (A) performed during the...
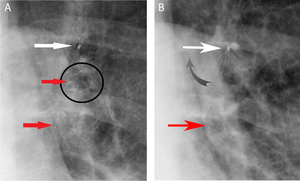
 shows three bronchial valves in the left upper lobe, respectively two Zephyr valves (red arrows) and one Spiration (white arrow). (B) Magnification of chest X-ray depicts the migration of a Zephyr valve (black circled in A), which cannot be seen; indeed, the patients reported the expulsion of the valve during cough.")
Fig. 12:
Expulsion of an endobronchial valve: magnification of chest X-ray (A) shows...
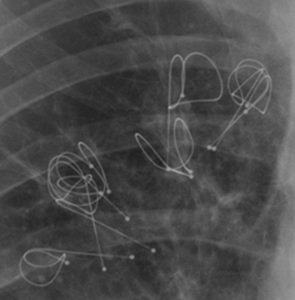
: chest X-ray magnification shows LVRC RePneu coils (PneumRx, Inc., Mountain View, CA, USA) in right upper lobe. LVRC are wires made of Nitinol, a nickel and titanium alloy that combines memory shape effects, strength, and elasticity. Up to 10 LVRCs can be positioned into the target lobe during a single procedure.")
Fig. 13:
Lung volume reduction coil (LVRC): chest X-ray magnification shows LVRC RePneu...
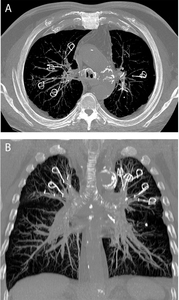
 reconstructed images in the axial (A) and coronal (B) plane of a patient with severe upper lobe predominant emphysema treated with bilateral positioning of LVRC. Pulmonary volume loss was achieved without atelectasis, which is a rare finding after LVRC indeed.")
Fig. 14:
Lung volume reduction with coils: maximum intensity projection (MIP)...

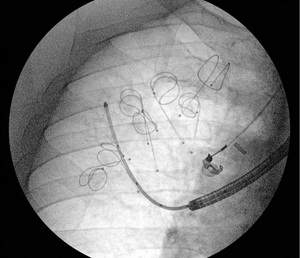
Fig. 15:
LVRC positioning: fluoroscopic image shows seven LVRCs in the right upper lobe...

Fig. 16:
Pattern of emphysema: volume rendering reconstruction of volumetric CT shows...
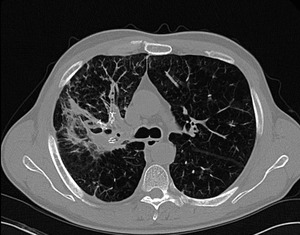
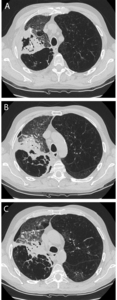
 in the follow-up of LVRC shows subtotal opacification of the right upper lobe. Opacification after LVRC positioning is an uncommon finding after LVRC, that can reflect either atelectasis (extremely rare) or pneumonia. In this case, the irregular morphology of the consolidation and air collections are consistent with pneumonia.")
Fig. 17:
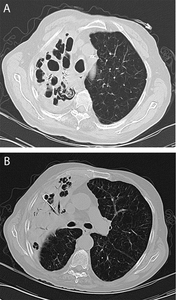
Pneumonia after coils lung volume reduction: axial chest CT with lung window...
 show synchronous consolidation and pneumothorax (white arrow) after LVRC positioning. Pneumothorax and infectious complications are the most frequent complications after LVRC or EBV.")
Fig. 18:
Multiple synchronous complications after LVRC: axial chest CT images with lung...