ECR 2016 / C-2016
Sports imaging in Baku: similarities and differences between the first European games and the London olympics
This poster is published under an open license. Please read the disclaimer for further details.
Congress:
ECR 2016
Poster Number:
C-2016
Type:
Scientific Exhibit
Keywords:
Musculoskeletal soft tissue, Musculoskeletal joint, Musculoskeletal bone, Ultrasound, MR, CT, Diagnostic procedure, Athletic injuries, Workforce
Authors:
D. Remedios1, D. Shah1, L. K. Singh1, J. Teh2, N. Ridley3, R. Suleymanov4; 1Harrow/UK, 2Oxford/UK, 3Swindon/UK, 4Baku/AZ
DOI:
10.1594/ecr2016/C-2016
 of investigations were needed between 9am and 9pm. An on-call radiologist was able to handle the small number of out-of-hours imaging. (Chart courtesy of Luis Moreno, First Solutions, PT.)")
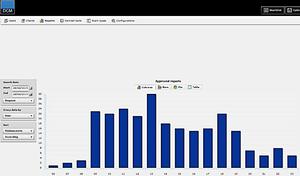
Fig. 1:
Fig 1. Baku imaging numbers displayed by the hour of the day. The majority...
")
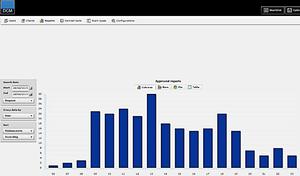
Fig. 2:
Fig 2. Baku imaging numbers displayed by the day during the three weeks that...

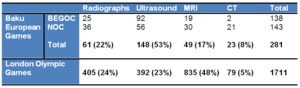
Fig. 3:
Fig 3. Baku European Games and the London Olympics: Comparison of imaging...

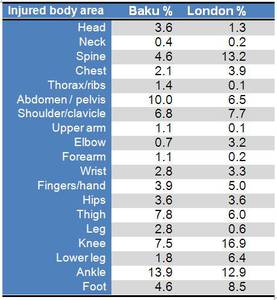
Fig. 4:
Fig 4. Baku European Games and the London Olympics: Comparison of body areas...

Fig. 5:
Gymnast: fall from the rings. STIR MRI sequence showing a grade 3 complete...

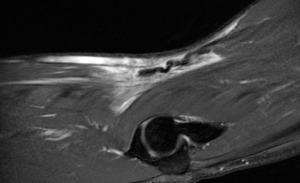
Fig. 6:
Grade 3 tear of the right adductor longus tendon from its origin in a long...

Fig. 7:
Endurance athlete: Grade 4 chronic bone stress fracture of the right proximal...
.")
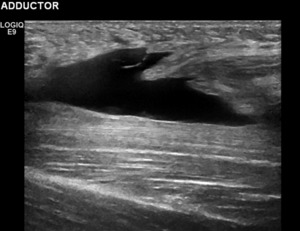
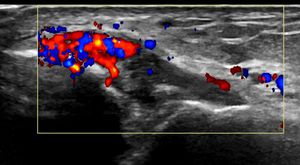
Fig. 8:
Hurdler: Inversion ankle injury. Colour flow ultrasound showing a Grade 2...

Fig. 9:
Fig 5. Baku European Games and the London Olympics: Similarities and...