In the Emergency Department “nothing as it seems”: about 10% of female patients with clinical diagnosis of acute appendicitis presented instead a gynecological pathology [ 1].
Moreover up to 13% women,
who present to General Surgeon having symptoms of acute abdomen,
have gynecological problems [2].Diagnosis of acute appendicitis often relies on clinical/laboratory data and on useful score (Alvarado score),
which summarizes clinical features,
(Table 1).
Ultrasound has 60–80% sensitivity and specificity for acute appendicitis and cannot be relied upon.
The report often states that they could not find anything in the right lower quadrant pain.
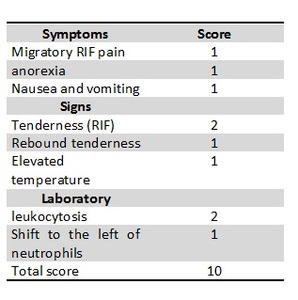
Table 1: ALVARADO SCORE
Interpretation of “Alvarado score” is as follows:
0–4 unlikely to be appendicitis
5–6 consistent with a diagnosis of appendicitis
7–8 probable appendicitis
9–10 very probable appendicitis
Even if the Alvarado score has reasonable rates of sensitivity and specificity –the literature suggests it is less reliable in young women: Symptoms/signs of appendicitis are similar to many Gynecological disorder.
The most important laboratory investigations are White Blood Cell Count (WBC) and C-reactive protein (CRP).
Acute appendicitis is typically characterized by increased WBC and CRP but in the early stages,
WBC and CRP can be normal for both.
On the other hand,
if the patient has had pain for more than two days and the CRP is normal,
the chances of appendicitis are almost nil,
remembering that there is an up to 48-hour lag in the CRP rising in response to inflammation.
Moreover,
not only appendicitis can hide gynecological pathologies: especially in young women,
radiologist have not to forget gynecological pathologies ( Table 2 ) as adnexal torsion,
ovarian cyst rupture or hemorrhage,
Mittelschmerz,
pelvic inflammatory disease (PID),
endometriosis and iatrogenic uterine perforations by non-medical illegal abortionists.
Table 2: Gynecologycal Acute Abdomen Aetiology in decescending order of frequency.
Complete assessment of these patients is required: they have to be correctly interviewed about the onset of the abdominal pain especially in relation with their cycle phase.
Essential for the correct diagnosis are WBC count,
pregnancy test,
Beta- HCG and serum CA 125,
if needed.
Radiologist should be more familiar with relationship between gynecological pathologies and cycle phase or Beta- HCG levels because this type of knowledge could help to arrive at the correct diagnosis.
For this reason,
we review gynecological pathologies dividing into the following group:
1) Pregnant related pathologies:
a. ECTOPIC pregnancy
2) Non pregnant related pathologies
a. Menstrual related: Endometriosis
b. Ovulation related:
i. Mittelschmerz
ii. Bleeding/rupture follicle
c. Non menstrual related:
i. Pelvic inflammation disease (PID)
ii. Ovarian torsion
iii. Ovarian adnexal mass

