PNEUMOTHORAX (PNX)
Pnx is defined as the presence of air or gas in the pleural cavity (the virtual space between the visceral and parietal pleura of the lung),
which can impair oxygenation and/or ventilation.
The clinical manifestations depend on the degree of collapse of the lung on the affected side.
If the pnx is significant,
it can cause a shift of the mediastinum and compromise hemodynamic stability.
We recognize different types of pnx:
- Spontaneous pneumothorax (PSP)
PSP,
as defined,
occurs in patients without underlying pulmonary disease.
Often these patients have asymptomatic blebs and bullae.
Fig. 1 PSP is typically observed in tall,
young people without parenchymal lung disease and it is thought to be related to increased shear forces in the apex[1].
Despite the presence of pleural blebs,
the exact anatomic site of air leakage is difficult to determine.
Fluorescein-enhanced autofluorescence thoracoscopy (FEAT) is a possible method to locate the site of air leak in PSP [2].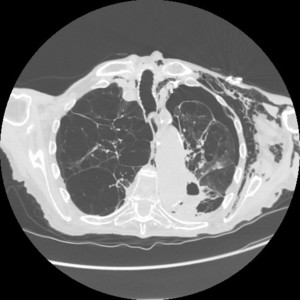
Fig. 1: Left pneumothorax, pneumomediastinum and subcutaneous emphysema in a man with severe diffuse bullous dystrophy of the lung. Rupture of a subpleural bulla caused pneumothorax.
Pathophysiology: In normal respiration,
the pleural space has a negative pressure.
As the chest wall expands outward,
the surface tension between the parietal and visceral pleura expands the lung outward.
The lung tissue intrinsically has an elastic recoil,
tending to collapse inwards.
If the pleural space is invaded by gas from a ruptured bleb,
the lung collapses until equilibrium is achieved or the rupture is sealed.
The main physiologic consequence of this process is a decrease in vital capacity and partial pressure of oxygen.
Many evidences suggest that genetic factors may be important ( Marfan syndrome,
homocystinuria,
and Birt-Hogg-Dube syndrome).
In the Birt-Hogg-Dube syndrome benign skin tumors (hair follicle hamartomas),
renal and colon cancer,
and spontaneous pneumothorax are associated (PSP occurs in about 22% of these patients) [3].
Also lung inflammation and oxidative stress are supposed to be important for the pathogenesis of PSP; in fact current smokers have an increased numbers of inflammatory cells in the small airways and have an increased risk for PSP .[4]
Iatrogenic pneumothorax is a complication of medical or surgical procedures.
The leading cause is transthoracic needle aspiration followed by therapeutic thoracentesis,
pleural biopsy,
central venous catheter insertion,
transbronchial biopsy,
positive pressure mechanical ventilation and inadvertent intubation of the right mainstem bronchus [5;6] .
The following list summarizes the main causes:
• Transthoracic needle aspiration biopsy of pulmonary nodules (most common cause,
32-37%) Fig. 2
• Transbronchial or pleural biopsy Fig. 3
• Thoracentesis
• Central venous catheter insertion,
usually subclavian or internal jugular vein
• Intercostal nerve block
• Tracheostomy
• Cardiopulmonary resuscitation (CPR) (consider the possibility of a pnx if ventilation becomes progressively more difficult).
• Acute respiratory distress syndrome (ARDS)
• Nasogastric feeding tube placement
Common causes of traumatic pneumothorax include:
• Trauma (penetrating and non-penetrating injury)
• Rib fracture
• High-risk occupation (diving,
flying)
Complications include hemopneumothorax,
bronchopleural fistula and tension pneumothorax.
Fig. 4
Tension pneumothorax: occurs anytime a disruption involves the visceral pleura,
parietal pleura,
or the tracheobronchial tree.
This condition develops when injured tissue forms a one-way valve,
allowing air inflow with inhalation into the pleural space and prohibiting air outflow.
The volume of non absorbable intrapleural air increases with each inspiration and,
as a result,
pressure rises within the affected hemithorax.
Moreover,
the positive pressure used by mechanical ventilation therapy can cause air trapping.
As the pressure increases,
the ipsilateral lung collapses and causes hypoxia.
Further pressure increase causes the mediastinum to shift toward the contralateral side and compress the controlateral lung: this rising pressure reduces the venous return to the right atrium,
causing impair cardiac function.
Hypoxia results as the collapsed lung on the affected side and the compressed lung on the contralateral side compromise effective gas exchange [7] Fig. 5
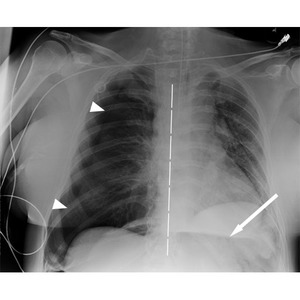
Fig. 5: Right tension PNX (arrowheads evidence pleural edge) with shifting of mediastinum to the opposite side (dashed line). An area of radiolucency on the left hypochondrium (arrow) suggest abnormal air in abdomen (also pneumoperitoneum and pneumoretroperitoneum were present). Same patient of Fig. 17 and Fig.18
Women aged 30-40 years with onset of symptoms within 48 hours of menstruation,
right-sided pneumothorax and recurrence [8] .
Radiological signs of pnx.
In chest radiograph a pneumothorax is demonstrate by:
-visible visceral pleural edge seen as a very thin,
sharp white line Fig. 6
-no lung markings are seen peripheral to this line
-the peripheral space is radiolucent compared to adjacent lung
-the lung may completely collapse
If a tension pneumothorax is present,
a mediastinum shift away from the pneumothorax is seen.
Fig. 4 Fig. 5
Radiograph is performed in lateral decubitus with the suspected side up: the lung will then 'fall' away from the chest wall.
In expiratory chest radiograph the lung becomes smaller and more dense while the pneumothorax remains the same size.
In CT scan we use lung window to search for pneumothorax.
When a bullous disease is present,
a loculated pneumothorax may appear similar.
Fig. 7
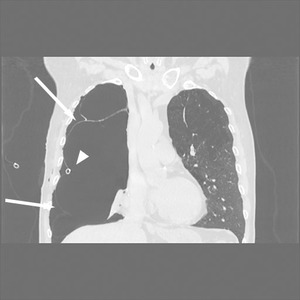
Fig. 7: CT scan shows some giant bullae of right lung that at the chest-Xray simulate a massive right pnx.
The bullous origin of the hypertrasparence on x-ray is confirmed by the position of drainage tube that is placed in the virtual pleural space (arrowhead). Arrows indicate visceral pleural line delimiting a giant bulla.
PNEUMOMEDIASTINUM
Pneumomediastinum is a condition in which air is present in the mediastinum,
where free air is not present normally.
This event can result from physical trauma or other situations that lead to air escaping from the lungs,
airways or bowel into the chest cavity.
Mediastinal Anatomy
The mediastinum is the mass of tissues and organs which divides the two pleural sacs,
located between the sternum in front and the vertebral column behind and extending from the thoracic inlet above to the diaphragm below.
The mediastinum is traditionally divided in: Table 1
-anterior compartment (prevascular space): includes the thoracic contents anterior to the pericardium: the thymus,
substernal extention of the thyroid,
blood vessels and lymph nodes;
-middle compartment (vascular space): includes the pericardium and its contents with the great vessels
-posterior compartment (postvascular space): contains trachea,
oesophagus,
descending aorta,
azygous vein,
nerves and lymph nodes.
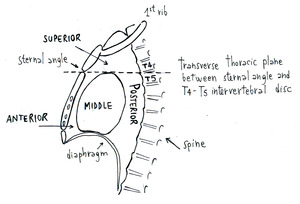
Table 1: Mediastinal anatomy.
The mediastinum communicates with several anatomic structures including the submandibular space,
the retropharyngeal space,
and the vascular sheaths in the neck.
A tissue plane extends anteriorly from the mediastinum to the retroperitoneal space through the sternocostal attachment of the diaphragm.
This space is continuous with the flanks and extends to the pelvis.
The mediastinum also communicates directly with the retroperitoneum from the periaortic and periesophageal fascial planes [9].
The main sources of pneumomediastinum are:
-through the skin and the chest wall (in the setting of penetrating trauma);
-from a tear or defect in the oesophagus or the trachea;
-from the alveoli,
if the intra-alveolar pressure increases and induces air entry into interstitial tissue of the alveolar wall [10].
The following list summarize the main causes [11;12;13;14] :
• blunt or penetrating chest trauma
• thoracic,
neck or retroperitoneal surgery
• oesophageal perforation (Boerhaave syndrome Fig. 8 ,
endoscopic intervention,
oesophageal carcinoma)
• tracheobronchial perforation or laceration,
bronchial stump dehiscence,
bronchoscopy,
tracheostomy,
laryngeal fracture
• vigorous exercise (pulmonary interstitial emphysema,
Valsalva maneuver)
• childbirth ( Hamman's syndrome mechanism)
• asthma (development of high intra-alveolar pressure in a lung unit behind an obstructed bronchus)
• barotrauma :diving,
ventilation (most commonly secondary to ARDS with positive pressure ventilation)
• infection (tuberculosis,
histoplasmosis,
dental or retropharyngeal infection ,
mediastinitis)
• idiopathic
Table 2
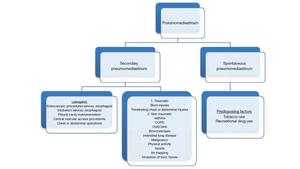
Table 2: Causes of pneumomediastinum.
References: VK. Kouritas, K. Papagiannopoulos, G. Lazaridis et al. (2015) Pneumomediastinum. J Thorac Dis 7(S1):S44-S49
With the accumulation of air in the mediastinum,
an increase in pressure could causes a decrease in venous retourn to the great veins,
resulting in cardiovascular impairment.
Howewer when pressure builds up within the mediastinum,
air usually dissects further along fascial planes into the neck,
allowing the release of the pressure and preventing serious cardiovascular complications.
In addition,
an increase in mediastinal pressure sometimes results in rupture of the mediastinal pleura and in the escape of air into the pleural space,
resulting in the development of a pneumothorax.
When air enters the the soft tissues of the neck,
the patient develops a subcutaneous emphysema that grows as the air continues to come from the mediastinum into the neck,
dissecting the soft tissues of chest and abdominal wall even more.
Thanks to the escape route available for mediastinal air and the opportunity for decompression,
major cardiovascular complications are quite uncommon.
The development of subcutaneous emphysema,
although unsightly and frequent uncomfortable,
is not associated with major clinical sequelae and,
even if very extended,
tends to resolve in weeks [10].
Spontaneous pneumomediastinum (described by Hamman in 1939) is considered when no apparent cause is identified.
It is more common in youngsters,
between the 2nd and the 4th decade,
especially in males.
Precipitating factors are cough,
labor or drug abuse.
The ‘Macklin effect’ establishes that the alveolar rupture caused by an increased intrathoracic pressure results in air dissecting the bronchovascular sheath until the mediastinum.
The Hammam’s syndrome (also known as Macklin's syndrome) is the association of spontaneous pneumomediastinum,
subcutaneous emphysema and in rare cases pneumorrachis.
The condition is most commonly asymptomatic.
Presenting symptoms can include non-specific chest pain,
dyspnoea,
dysphonia and fever.
On clinical examination,
we can find the ‘Hamman sign’ that consists in a pulse-synchronous rasping sound heard over the precordium in spontaneous mediastinal emphysema produced by the heart beating against air-filled tissues [15].
As already explained,
stretching of the mediastinal pleura by pneumomediastinum can lead to his rupture and to pnx.
Pneumomediastinum can lead also to pneumopericardium,
pneumoperitoneum or pneumoretroperitoneum [16].
Rarely,
the pressure in pneumomediastinum can be high enough to cause hypotension by impairing venous return to the heart,
in a tension pneumomediastinum setting.
Tension pneumomediastinum is caused by an important increase in intramediastinal pressure,
which results from accumulation of free air that may compress the heart,
causing a decrease in venous return and a compression of the tracheobronchial tree.
All of these changes may lead to sudden,
profound cardiovascular and respiratory collapse.
In these patients,
sudden development of severe hypoxia,
hypotension,
tachycardia,
metabolic acidosis,
and high ventilation pressure should be suspicious for tension in the mediastinum.This emergency situation requires prompt treatment such as percutaneous needle aspiration of mediastinal air in order to reverse cardiovascular and respiratory impairment [17].
The pneumomediastinum is basically a rare entity; the majority of patients are male (76% of cases).
However,
many authors believe that the occurrence of pneumomediastinum is more frequent than initially believed due to underdiagnosis,
with many patients refraining from medical help.
This illness may not be indentified on the chest radiograph and consequently related symptoms may be attributed to musculoskeletal pain or other insignificant causes .
Pneumomediastinum usually occurs in young patients,
maybe because the mediastinal tissues are loose and flaccid,
whereas in the elderly group the planes and sheaths are fibrous,
making air migration more difficult.
The main symptom is severe central chest pain,
usually retrosternal,
irradiating to the neck or the back.
Other symptoms include laboured and shortness breathing,
voice distortion and subcutaneous emphysema (that can be detected in 70% of patient with diagnosed pneumomediastinum),
specifically affecting the face,
neck,
and chest.
Clinical evaluation may also identify tachycardia,
tachypnea or anxiety.
symptoms mimicking cardiac tamponade as a result of the increased intrapulmonary pressure on venous flow to the heart can also be find [14].
Radiological signs of pneumomediastinum
On plain chest radiography: Fig. 9
-Thymic sail sign (in infants): the thymus becomes elevated and partly surrounded by air.
- “Ring around the artery” sign: air surrounding the pulmonary artery or its main branches.
- Tubular artery sign: Pulmonary air and pneumomediastinum surround the aorta and its main branches.
- Double bronchial wall sign: air outside and within the bronchial wall allows the wall to be seen.
- Continuous diaphragm sign: caused by air located behind the pericardium.
- Extrapleural sign (or Naclerio’s V sign): air outlines the lateral margin of the descending aorta and can extend laterally between the parietal pleura and the medial left hemidiaphragm.
This finding was originally described in association with esophageal rupture (such as Boerhaave syndrome,
in fact,
even if not specific,
it can be an early sign of oesophageal perforation in appropriate clinical situation )
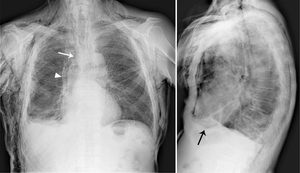
Fig. 9: Pneumomediastinum with subcutaneous emphysema. White arrow indicates air surronding trachea and bronchus that allows their wall to be seen.
Black arrow shows a thin radiolucent line between pericardium and diaphragm. If the air is located under the entire surface of the heart, the diaphragm will be seen entirely as in the "continuous diaphragm sign".
Arrowhead evidences the thickened mediastinal pleura, visible as an irregular line for the presence of air in the mediastinum; (this patient underwent a talc pleurodesis for a mesothelioma).
On CT scan pneumomediastinum findings are:
-lucent streaks or bubbles of gas that outline mediastinal structures,
elevate the mediastinal pleura,
and often extend into the neck or chest wall
-gas outlines the inner surface of the mediastinal pleura,
creating a visible pleural line lateral to the main pulmonary artery and the aortic arch; this pleural line is composed of both the parietal pleura of the mediastinum and the visceral pleura of the lung. Fig. 10
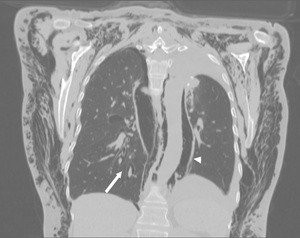
Fig. 10: Air around pulmonary vessels and bronchi on the right side (arrow) and surrounding the entire descending aorta and posterior mediastinal structures (arrowhead).
Dependent location of gas and visible webs of connective tissue outside pleural line help distinguish extrapleural gas from pneumothorax. Fig. 11 Fig. 12
In the emergency condition of a tension pneumomediastinum,
CT is the modality of choice and shows:
-substantial mediastinal free air,
-flattening of the anterior cardiac contour and compression of the right atrium, Fig. 13
-uplifting of the heart off of the diaphragm,
-distention of the inferior vena cava,
-compression of the mediastinal vessels and flattening of the main bronchi.
Fig. 14

Fig. 13: Massive subcutaneous emphysema with a large amount of air around mediastinal structures determining flattening of the anterior cardiac contour (arrowheads) and compression of the right atrium.
We also need to distinguish pneumomediastinum from pneumopericardium.
The first consideration is that pneumomediastinum is much more common,
except in case of recent heart surgery.
Pneumomediastinum usually manifests itself as a multitude of thin streaks,
the gas seldom surrounds the heart completely,
nor is confined to the region around the heart.
Instead in pneumopericardium:
- usually there is a single band of gas that may outline both the left ventricle and the right atrium,
-this band can be broad,
curved and sharply demarcated by the pericardial sac,
-it does not extend into the upper mediastinum or neck [16;17].
SUBCUTANEOUS EMPHYSEMA
Subcutaneous emphysema refers to air in the subcutaneous tissues of the body wall or limbs,
because air often dissects into the deeper soft tissues and musculature along fascial planes.
Causes of subcutaneous emphysema can be divided into:
-gas arising internally: pneumothorax,
pneumomediastinum,
pulmonary interstitial emphysema,
perforated hollow viscus in the neck,
oesophageal perforation,
fistula tract
-gas introduced externally: penetrating trauma,
post-surgical,
post-percutaneous intervention (such as pleural drain insertion)
-gas produced de novo: gas producing infections (necrotising fasciitis)
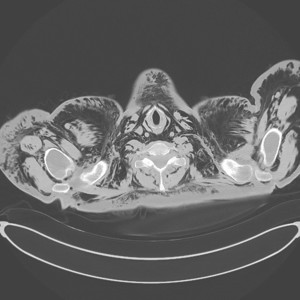
Fig. 15: Massive subcutaneous emphysema of neck and upper thorax after lung surgery; also pneumomediastinum is associated.
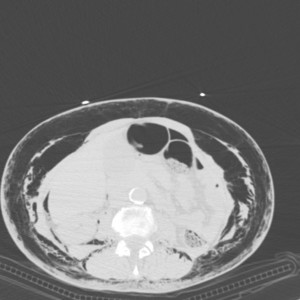
Fig. 16: After lung surgery, subcutaneous emphysema spreads from the thorax (see also Fig 11 and Fig 12) to the abdomen wall. A few quantity of gas is present also in peritoneum.
Clinically it is felt as crepitus and,
if extensive,
may cause soft tissue swelling and discomfort.
Even if severe subcutaneous emphysema is typically benign,
complications such as airway impairment,
respiratory failure,
pacemaker malfunction and tension phenomena have been described.
In the trauma situation,
the gas often doesn’t need treatment,
but its importance lies in the fact that its presence indicates possible serious injuries that could require urgent management.
Air can track along fascial planes and enter the head,
neck,
limbs,
chest,
abdomen,
and scrotum.
[11;18;19;20]
Fig. 17 Fig. 18
Radiological sign of subcutaneous emphysema:
On plain chest radiography there are often striated lucencies in the soft tissues that may outline muscle fibers.
If affecting the anterior chest wall,
subcutaneous emphysema can outline the pectoralis major muscle,
giving rise to the ginkgo leaf sign (when air outlines the fibers of the pectoralis major muscle and creates a branching pattern it resembles the branching pattern in the veins of a ginkgo leaf).
Fig. 19
On chest CT subcutaneous emphysema is readly visible,
with pockets of air seen as extremely dark low attenuation areas in the subcutaneous space [11].

Fig. 19: "Ginko leaf sign" in a patient with subcutaneous emphysema (and pneumomediastinum) after positioning of chest tube for right pnx. Same patient of Fig.3.




 which assumes a characteristic horizontal air-fluid level:hematic hydropneumothorax.
The heart and other mediastinal structures are shifted to the left, in a setting of hypertensive pnx.
A drainage tube was placed in the right pleural space to drain air and fluid (arrow).")
 with shifting of mediastinum to the opposite side (dashed line). An area of radiolucency on the left hypochondrium (arrow) suggest abnormal air in abdomen (also pneumoperitoneum and pneumoretroperitoneum were present). Same patient of Fig. 17 and Fig.18")

. Arrows indicate visceral pleural line delimiting a giant bulla.")

 Pneumomediastinum. J Thorac Dis 7(S1):S44-S49")

.")
 and surrounding the entire descending aorta and posterior mediastinal structures (arrowhead).")
. On the right side, extrapleural gas is distinguished from pnx for the presence of visible webs of connective tissue outside pleural line (arrow).")
on the right and pnx (arrowhead) on the left.")
 and compression of the right atrium.")
.")

 to the abdomen wall. A few quantity of gas is present also in peritoneum.")
. See also Fig 5.")

 after positioning of chest tube for right pnx. Same patient of Fig.3.")
