ECR 2017 / C-1206
Acute pancreatitis: a pictorial review
This poster is published under an open license. Please read the disclaimer for further details.
Congress:
ECR 2017
Poster Number:
C-1206
Type:
Educational Exhibit
Keywords:
Pancreas, CT, MR, Ultrasound, Diagnostic procedure, Education, Structured reporting, Education and training, Inflammation, Acute
Authors:
P. Tarcău, M. D. COMSA; Cluj-Napoca/RO
DOI:
10.1594/ecr2017/C-1206
 with normal pancreatic enhancement and no collections. References: Department of Radiology, Regional Institute of Gastroenterology and Hepatology, Cluj-Napoca/Romania 2016")
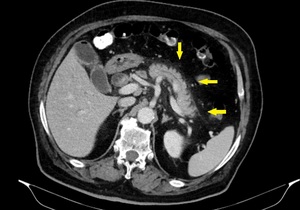
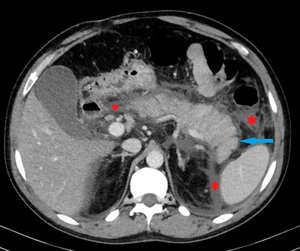
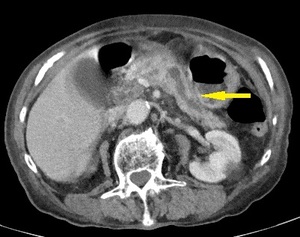
Fig. 1:
IEP in a 77-year-old man with gallstone-related pancreatitis. Axial...
 and peripancreatic haziness (yellow arrow). References: Department of Radiology, Regional Institute of Gastroenterology and Hepatology, Cluj-Napoca/Romania 2016")
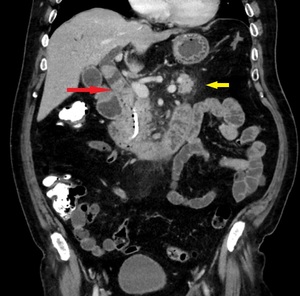
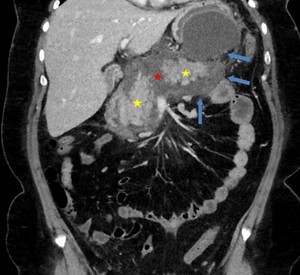
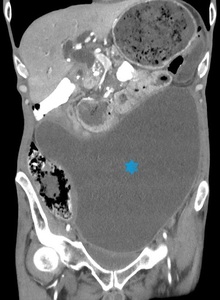
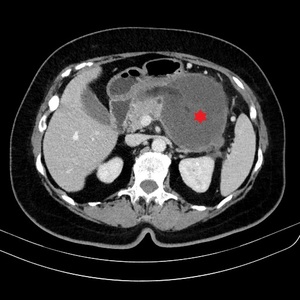
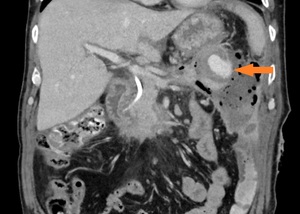
Fig. 2:
Same patient as in Fig. 1. Coronal image shows the choledocholithiasis (red...
 and minimal peripancreatic fluid collection (red star). References: Department of Radiology, Regional Institute of Gastroenterology and Hepatology, Cluj-Napoca/Romania 2016")
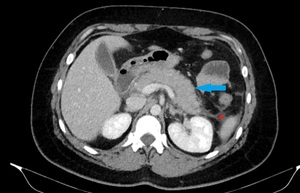
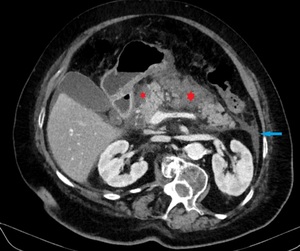
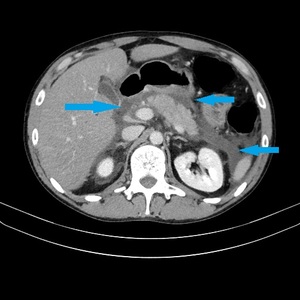
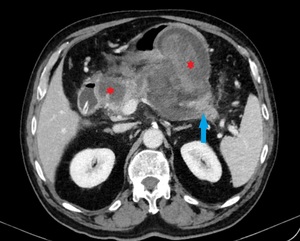
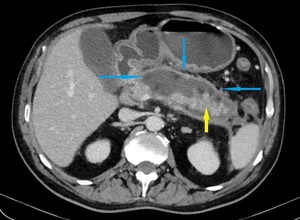
Fig. 3:
IEP in a 30-year-old woman. Axial contrast-enhanced CT image shows enlargement...
. Enlargement of the pancreas with normal enhancement (blue arrow) and minimal peripancreatic fluid collection (red star). References: Department of Radiology, Regional Institute of Gastroenterology and Hepatology, Cluj-Napoca/Romania 2016")
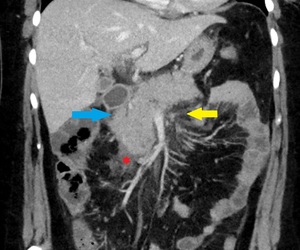
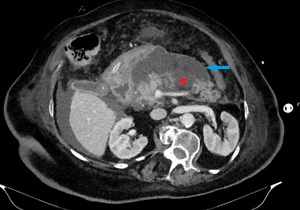
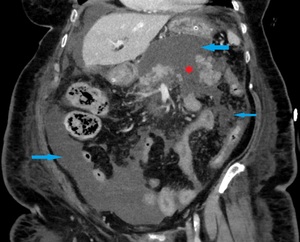
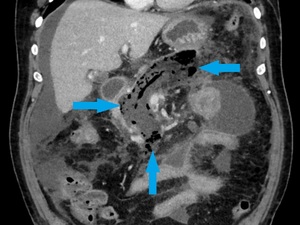
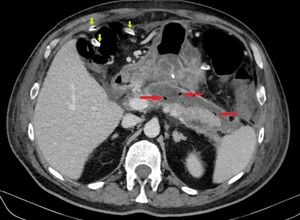
Fig. 4:
Same patient as in Fig. 3. Fat stranding (yellow arrow). Enlargement of the...
 and homogeneous fluid-attenuation collections adjacent to the pancreas, anterior to the left pararenal fascia and in the left paracolic gutter space (red stars), findings that are consistent with APFCs. References: Department of Radiology, Regional Institute of Gastroenterology and Hepatology, Cluj-Napoca/Romania 2016")
Fig. 5:
IEP in a 41-year-old man. Axial contrast-enhanced CT image shows normal...
, normal enhancement of the head and body (yellow stars) and peripancreatic heterogeneous collection (blue arrows), a finding consistent with ANC. References: Department of Radiology, Regional Institute of Gastroenterology and Hepatology, Cluj-Napoca/Romania 2016")
Fig. 6:
Necrotising pancreatitis in a 37-year-old woman. Coronal contrast-enhanced CT...
 and a collection in the left anterior pararenal space (blue arrow). References: Department of Radiology, Regional Institute of Gastroenterology and Hepatology, Cluj-Napoca/Romania 2016")
Fig. 7:
Necrotising pancreatitis in a 79-year- old woman. Axial CECT image shows...
, collections distributed in the entire abdomen (blue arrows) and the presence of a gallstone (green arrow). References: Department of Radiology, Regional Institute of Gastroenterology and Hepatology, Cluj-Napoca/Romania 2016")
Fig. 8:
Same patient as in Fig. 7. Multiple areas of abnormal pancreatic enhancement...
 and a heterogeneous collection containing both fluid and non-fluid densities (blue arrow), a finding that is consistent with ANC. References: Department of Radiology, Regional Institute of Gastroenterology and Hepatology, Cluj-Napoca/Romania 2016")
Fig. 9:
Same patient as in Fig. 7. Image acquired after 2 weeks shows the progression...
 and heterogeneous collections containing both fluid and non-fluid densities (blue arrows), a finding that is consistent with ANCs. References: Department of Radiology, Regional Institute of Gastroenterology and Hepatology, Cluj-Napoca/Romania 2016")
Fig. 10:
Same patient as in Fig. 7. Coronal image acquired after 2 weeks shows the...
, marks of APFCs. References: Department of Radiology, Regional Institute of Gastroenterology and Hepatology, Cluj-Napoca/Romania 2016")
Fig. 11:
IEP in a 26-year-old man. Axial contrast-enhanced CT image shows homogeneous...
 that are confined by the normal anatomical fascial planes. These findings are consistent with APFCs. References: Department of Radiology, Regional Institute of Gastroenterology and Hepatology, Cluj-Napoca/Romania 2016")
Fig. 12:
Same patient as in Fig. 11. Coronal contrast-enhanced CT image shows...
. References: Department of Radiology, Regional Institute of Gastroenterology and Hepatology, Cluj-Napoca/Romania 2016")
Fig. 13:
Pseudocyst in a 50-year-old man with recurring pancreatitis. The fluid...
 in an 87-year-old woman with recurring pancreatitis. References: Department of Radiology, Regional Institute of Gastroenterology and Hepatology, Cluj-Napoca/Romania 2016")
Fig. 14:
Pseudocyst (blue star) in an 87-year-old woman with recurring pancreatitis.
, markers of recurring pancreatitis. References: Department of Radiology, Regional Institute of Gastroenterology and Hepatology, Cluj-Napoca/Romania 2016")
Fig. 15:
Same patient as in Fig. 14. Dilatation and strictures of the main duct (yellow...
. References: Department of Radiology, Regional Institute of Gastroenterology and Hepatology, Cluj-Napoca/Romania 2016")
Fig. 16:
WON in a 65-year-old woman with necrotising pancreatitis. Axial CECT image...
 and several heterogeneous collections containing non-liquefied debris (red stars). References: Department of Radiology, Regional Institute of Gastroenterology and Hepatology, Cluj-Napoca/Romania 2016")
Fig. 17:
WON in an 80-year-old man with pancreatic parenchyma necrosis greater than 30%...
. References: Department of Radiology, Regional Institute of Gastroenterology and Hepatology, Cluj-Napoca/Romania 2016")
Fig. 18:
Infected WON in a 63-year-old man. Coronal image shows the infected WON...
, markers of gas-producing bacteria. References: Department of Radiology, Regional Institute of Gastroenterology and Hepatology, Cluj-Napoca/Romania 2016")
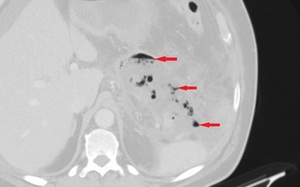
Fig. 19:
Axial image of the same patient as in Fig. 18. Lung window highlights the gas...
 attenuation densities (blue arrows) and an enhancing remainder of pancreatic parenchyma (yellow arrow). References: Department of Radiology, Regional Institute of Gastroenterology and Hepatology, Cluj-Napoca/Romania 2016")
Fig. 20:
Complications in a 64-year-old man with necrotising pancreatitis.
Axial CECT...
 and percutaneous drainage catheters (green arrows). References: Department of Radiology, Regional Institute of Gastroenterology and Hepatology, Cluj-Napoca/Romania 2016")
Fig. 21:
Same patient as in Fig. 20, after 2 weeks. ANC infection (gas bubbles – red...
. References: Department of Radiology, Regional Institute of Gastroenterology and Hepatology, Cluj-Napoca/Romania 2016")
Fig. 22:
Same patient as in Fig. 20, after another 5 weeks. Coronal CECT image shows a...