Perianal fistula
Perianal fistula is usually encountered in young adults [3].
It most commonly presents with discharge [4].
It is more common among men.
Possible underlying pathogenesis of perianal fistulas is proposed to be intersphincteric ductal obstruction with resultant anal gland infection and sepsis,
which is known to be ‘cryptoglandular hypothesis’.
In the first setting infection takes place in the intersphincteric space which is the most common location and presentation for idiopathic fistulas.
Though usually primary in origin,
Crohn’s disease,
pelvic surgery,
tuberculosis and pelvic malignancies may be an underlying cause of perianal fistulas [5].
MRI is accepted as the choice of imaging modality for radiological evaluation of perianal fistulas as well as radiological follow-up [6].
Perianal fistula is a clinical entity notorious for recurrences in cases of inadequate or inaccurate medical or surgical treatment.
Preoperative radiological evaluation via MRI helps to distinguish the type of fistula,
its internal opening,
possible associated abscesses and secondary tracts as clinically concealed sites of sepsis and common reasons of recurrence [4].
MRI has a superiority over clinical examination since it can seperate only active inflammation from accompanying fistulous tracts when both are similar on palpation [7].
Main disadvantages of MRI are that it is expensive,
time consuming due to relatively long scan times and difficult to perform in claustrophobic patients.
Grading of perianal fistulas was revised with respect to MRI findings by St.
James classification into five distinct grades with increasing grades correlating to worse surgical results: grade 1 for intersphincteric fistulas,
grade 2 for intersphincteric fistulas with abscesses or secondary tract,
grade 3 for transsphincteric fistulas,
grade 4 for transsphincteric fistulas with abscesses or secondary tract and grade 5 for supralevator fistulas [8].
In grade 1 fistulas,
tract extends from skin to anal canal traversing through intersphincteric plane (Figure 1).
If fistulas with same trajectory are associated with abscesses or secondary branches within intersphincteric plane they are upgraded to grade 2 (Figure 2).
Grade 3 fistulas extend through both internal and external sphincters -so called transsphincteric- fistula (Figure 3).
When additional ischioanal fossa abscess or secondary tract is present,
they are accepted as grade 4 fistula (Figure 4).
Grade 5 fistulas pose a different pathogenetic mechanism as they are not related to intersphincteric plane and dentate line; they breach levator muscle through their courses and are related with pelvic infectious foci (Figure 5).
Internal opening of fistulas are described according to clock system in lithotomy position; 12 o’clock denoting anterior,
6 o’clock posterior.
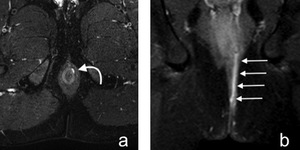
Fig. 1: Figure 1. Grade 1 perianal fistula. Axial fat suppressed T2-weighted (a) and coronal postcontrast T1-weighted (b) images show grade 1 simple intersphincteric fistula (curved and straight white arrows). There is no secondary extension or associated abscess cavity.
References: Hacettepe University/ Ankara - Turkey

Fig. 2: Figure 2. Grade 2 perianal fistula. Coronal fat suppressed T2-weighted (a) and postcontrast T1-weighted (b) images reveal intersphincteric fistula (curved white arrows) and related abscess cavities (white arrows) with varying sizes. Abscess cavities exhibit hyperintensity on T2-weighted image and peripheral rim type contrast enhancement on postcontrast T1-weighted image. Patient had accompanying Crohn’s disease.
References: Hacettepe University/ Ankara - Turkey
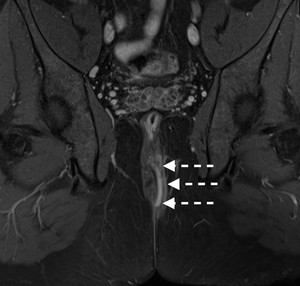
Fig. 3: Figure 3. Grade 3 perianal fistula. Coronal fat suppressed T2-weighted image demonstrates fistulous tract (dashed white arrows) traversing both sphincters compatible with transsphincteric fistula.
References: Hacettepe University/ Ankara - Turkey
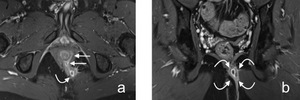
Fig. 4: Figure 4. Grade 4 perianal fistula. Axial (a) and coronal (b) postcontrast T1-weighted images show grade 4 transsphincteric fistula (straight white arrows) with accompanying abscess cavity in left ischioanal fossa (curved white arrows).
References: Hacettepe University/ Ankara - Turkey

Fig. 5: Figure 5. Grade 5 perianal fistula. Axial postcontrast T1-weighted image demonstrates left grade 5 supralevator fistula (white arrows).
References: Hacettepe University/ Ankara - Turkey
Hidradenitis suppurativa
Hidradenitis suppurativa (HS) is a chronic disease usually coursing with recurrences [9].
It mainly affects hair follicles and apocrine glands; axillary and inguinal regions are most frequently involved.
Inguinoperineal involvement is more frequently encountered among men [10].
When pathogenesis of HS is considered,
apocrine gland involvement is supposed to be a secondary event; mainly due to occlusion of hair follicle [11,
12] .
Inguinoperineal involvement may present with local pain,
discharge and bleeding.
Untreated or chronic recurrent disease may end up with anal or urethral strictures.
MRI has an adjunctive role as exhibiting extent of inflammatory changes,
subcutaneous thickening as well as associated sinus tracts and abscesses [10].
Skin and subcutaneous changes are most prominent around perineum and medial thigh.
Since inflammation is the underlying pathogenesis,
they are seen as hypointense on T1-weighted images,
hyperintense on T2-weighted and STIR images (Figure 6).
Additionally abscess cavities exhibit peripheral enhancement on postcontrast T1-weighted images.
Lack of enteral communication is a key feature for separating HS from perianal fistulas since extension to sphincter complex is rare in HS.
[12].
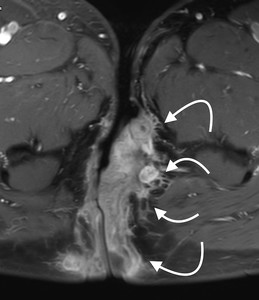
Fig. 6: Figure 6. Hidradenitis suppurativa. Axial postcontrast T1-weighted image shows bilateral marked thickening of skin and subcutaneous tissues with accompanying contrast enhancement (curved white arrows) in a patient with inguinoperineal hidradenitis suppurativa.
References: Hacettepe University/ Ankara - Turkey
Pilonidal sinus
Pilonidal sinus is caused by inflammatory process located at natal cleft reactive to the hair follicle which causes a foreign body reaction around.
With subsequent folliculitis,
abscess and sinus tract formation more hair follicles are involved in ongoing inflammatory process.
Pilonidal sinus is most commonly encountered among young adults.
It usually presents with fever,
pain and discharge though presentation is variable depending on the stage of inflammation [13].
Location of pilonidal sinus far from and posterior to anal canal at natal cleft is clinically pathognomonic and distinctive from perianal fistulas.
In the vast majority of cases inflammatory changes are superficial and involve tissues around coccyx and sacrum (Figure 7).
In complex and recurrent cases detection of intersphincteric changes are key for differential diagnosis since it invariably points to presence of perianal fistulas [14].
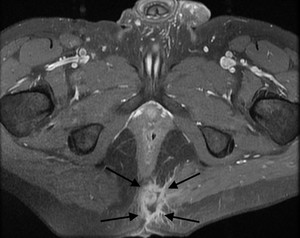
Fig. 7: Figure 7. Pilonidal sinus. Axial postcontrast T1-weighted image reveals peripherally enhancing pilonidal sinus (black arrows). Sinus tract has communication with skin at natal cleft level.
References: Hacettepe University/ Ankara - Turkey
Rectovaginal/anovaginal fistula
The leading cause of recto/anovaginal fistulas is trauma due to obstetric reasons,
followed by Crohn’s disease and pelvic radiotherapy [15].
They may cause debilitating symptoms such as feces and/or flatus discharge from vagina and recurrent vaginal infections [16].
Imaging of these fistulas pose a challenge even with most complicated multiplanar and sectional imaging techniques and subtle fistulas without accompanying secondary abnormalities may easily be missed.
On MRI rectovaginal/anovaginal fistulas are seen as tiny hyperintense tracts on T2-weighted images.
Accompanying presence of air both in fistulous tract and rectovaginal septum is an important imaging clue for diagnosis [15].
In advanced cases accompanying dense inflammatory changes and small abscess cavities in vicinity especially in rectovaginal septum may be encountered,
even they may render visualisation of original fistulous tract impossible.
Abscess cavities located in rectovaginal septum present with typical hypointense signal on T1-weighted images and hyperintense signal on T2-weighted images and exhibit peripheral contrast enhancement,
if postcontrast examination is done (Figure 8).
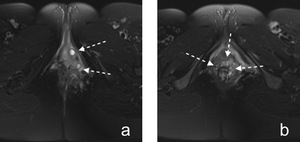
Fig. 8: Figure 8. Rectovaginal fistula. Axial fat suppressed T2-weighted images (a,b) passing through different levels show abscesses and thickening of rectovaginal septum consistent with rectovaginal fistula (dashed white arrows). There are hazy surrounding increased signal intensity due to inflammatory changes.
References: Hacettepe University/ Ankara - Turkey
Anal canal carcinoma
Anal canal carcinoma is a rare malignancy which constitutes about 2.5 % of all colorectal carcinomas [17].
Its most common histological subtype is squamous cell carcinoma.
Patients usually present with local pain,
pruritus,
rectal bleeding,
conspitation and frank mass.
Lymphatic spread route of anal canal carcinomas differ with respect to location of lesions: Lesions below dentate line to inguinal nodes,
lesions above dentate line to internal iliac,
perirectal and mesorectal nodes [18].
Anal canal carcinomas are visualised as hyperintense lesions on T2-weighted images [19].
MRI reveals extension of tumor into internal,
external sphincters and if present,
into anterior urogenital triangle,
ischioanal fossa.
They are seen as asymmetric thickening and stranding of involved soft tissues (Figure 9).
MRI is also shown to be useful for follow-up of anal canal carcinomas following chemoradiotherapy.
Tumor regression with respect to size is accompanied by decreased signal intensity on T2-weighted images when compared to initial imaging studies [19].
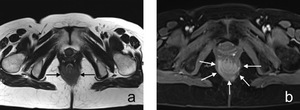
Fig. 9: Figure 9. Anal canal carcinoma. Axial precontrast (a) and postcontrast (b) T1-weighted images demonstrate irregular mass lesion (white arrows) involving sphincter complex and mostly posterior half of anal canal. Mass lesion exhibits avid enhancement on postcontrast image.
References: Hacettepe University/ Ankara - Turkey
Anal fissure
Anal fissure is a commonly encountered condition which may have debilitating symptoms including painful defecation and rectal bleeding.
Constipation and increased anal muscle tone are considered as possible underlying pathogenetic mechanisms in development of anal fissures.
It is mostly seen in posterior midline and characterized by a split in distal anoderm (Figure 10).
Some patients may heal spontaneously or with help of medical and/or surgical treatment meanwhile the condition becomes chronic in some patients.
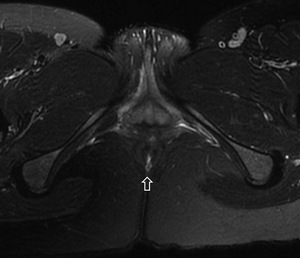
Fig. 10: Figure 10. Anal fissure. Axial postcontrast T1-weighted image demonstrates anal dermal split at posterior midline location consistent with anal fissure (empty arrow).
References: Hacettepe University/ Ankara - Turkey
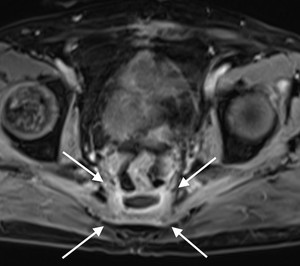
Fig. 11: Figure 11. Presacral abscess. Axial postcontrast T1-weighted image shows peripheral rim enhancement of presacral abscess. Patient had history of recent abdominoperineal resection.
References: Hacettepe University/ Ankara - Turkey
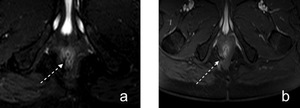
Fig. 12: Figure 12. Postsurgical defect at anal sphincter. Axial fat suppressed T2-weighted (a) and postcontrast T1-weighted (b) images demonstrate focal defect located in external sphincter around 6-8 o’clock (dashed white arrows) in a patient with history of perianal fistula surgery.
References: Hacettepe University/ Ankara - Turkey
