1.
Prostatic mpMRI technique
Patient preparation:
- Antispasmodic agents - recommended but not obligatory (adverse effects)
- Previous evacuation
- Ventral decubitus may be indicated in the presence of rectal gas (reduces the artifacts)
NOTE: In the case of a prior biopsy,
haemorrhage may influence image interpretation,
specially when the mpMRI is performed for local staging (recommended interval of 6 weeks).
Technical considerations:
- Magnetic field 1.5T or 3T (preference for the 3T)
- Endorrectal antenna is not necessary
- More time and cost
- Deforms the gland
- More artifacts
- Patient discomfort
- All examinations must include: T1WI,
T2WI,
diffusion weighted imaging (DWI) and dynamic contrast-enhanced (DCE) sequences
- One sequence with a large FOV
- DWI b≥1400 (RSNA recommends: b10-50,
400,
800,
1200-1400)
2.
Image interpretation
T1 WI
- Determine the presence of postbiopsy haemorrhage
- Delineate the gland boundary
- Detection of nodal and skeletal metastases
T2 WI
- Zonal anatomy
- Assess abnormalities within the gland,
especially in the transition zone
- Local staging (seminal vesicles invasion; extra-prostatic extension)
The quality of these images should be as high as possible because they are the key images for detecting significant cancers,
especially in the TZ.
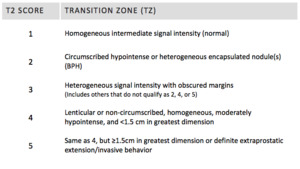
Fig. 2: T2 Score - Transition Zone
TZ lesions should be measured on T2W images.
DWI
- Peripheral zone evaluation
- Transition zone additional evaluation
DWI is a key component of prostate mpMRI examinations,
specially in the detection of significant cancers in the peripheral zone.
The ADC value of a focal tumour is inversely correlated with the Gleason pattern: The lower the ADC value,
the higher the Gleason pattern.
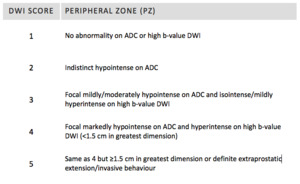
Fig. 3: DWI Score - Peripheral Zone
PZ lesions should be measured on ADC maps.
DCE
- Provide additional information if DWI is technically limited
- Detection of noneoplastic diseases (prostatitis)
- Kinetic evaluation is not recommended
- Alterations seen on parametric maps must be confirmed with the dynamic study and subtraction images
- DCE serves primarily to help detect significant PCa and not to characterise it.
Most published studies show that the added value of DCE over the combination of T2W and DWI is modest.
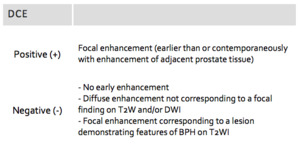
Fig. 4: DCE score
3.
PI-RADS Assessment
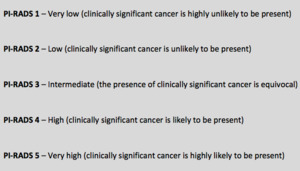
Fig. 6: PI-RADS classification
PI-RADS v2 uses a 5-point scale indicating the likelihood that mpMRI findings correlate with the presence of clinically significant PCa at a particular anatomic location ( Fig. 6 ).
Clinically significant disease is defined as Gleason score >7 (including 3 + 4 with prominent but not predominant Gleason grade 4),
and tumour volume >0.5 ml,
and/or extraprostatic extension.
Assignment of a PI-RADS assessment category for each lesion is based on the scoring of T2W,
DWI,
and DCE sequences performed sequentially according to zonal anatomy.
For the PZ,
DWI is the primary determining sequence.
For the TZ,
T2WI is the primary determining sequence.
The scoring for T2W and DWI uses a 5-point scale ( Fig. 2 and Fig. 3 ); for DCE,
a 2-point scale (present or absent) is used ( Fig. 4 ).
When T2WI and DWI are of adequate diagnostic quality,
DCE plays a minor role.
Although DCE has an importante role in the indeterminate category 3 PZ lesions,
it does not contribute to the overall assessment category when the findings suggest a low PI-RADS (1 or 2) or high PI-RADS (4 or 5).
When a PZ lesion has a DWI score of 3,
a positive DCE increases the likelihood that the finding corresponds to a clinically significant PCa and upgrades the assessment category to PI-RADS 4.
Benign prostatic hyperplasia (BPH) is intrinsically heterogeneous,
including ill-defined structures and those that are highly cellular and vascular.
This is why tumour detection in the TZ is less accurate compared with the PZ; the normal PZ has a more homogenous appearance.
Although T2W images are dominant in the TZ,
any lesion with low ADC and high signal intensity on high b-value images should be regarded with caution and should be carefully evaluated and biopsied if necessary.
In clinical practice,
visually bright foci in the TZ on high b-value DWI help draw the radiologist’s attention to a potential lesion and trigger more detailed analysis of this area using the rest of the MR data set.
In this sense,
initial localisation of the suspicious region using the b-value >1400 images can be useful in raising one’s confidence regarding the presence of a lesion,
even if the final PI-RADS category is largely determined by T2WI.
Location
All suspicious intraprostatic lesions seen on mpMRI should be assigned to their zonal location:
- Peripheral Zone (PZ)
- Transition Zone (TZ)
- Central Zone (CZ)
CZ,
like the TZ,
often shows hypointensity on T2WI and ADC and high signal on the high b-value images and thus may mimic significant PCa; therefore,
in PI-RADS v2,
this zone is separately indicated in the 39-sector scheme.
When there is more than one lesion,
the index lesion is by definition the one with the highest PI-RADS or the largest lesion if there is more than one with the same category.
If there are more than four suspicious findings,
only the four with the highest PIRADS should be reported.
Reporting of additional or definitely benign findings is optional but may be helpful to compare lesions on future examinations.
If a suspicious finding extends beyond the boundaries of one sector,
all neighbouring involved sectors should be indicated on the sector map as a single lesion.
A flowchart can be found on Fig. 7.
4.
Limitations,
frequent problems and future directions
PI-RADS v2 is exclusively based in the RM and does not evaluate detention of recurrence nor progression during active monitoring.
4.1.
Interreader agreement
Two initial studies of PI-RADS v2 (Muller BG et al,
2015; Vargas HA et al,
2015) reported moderate interreader agreement among readers from the same center and limited performance in the assessment of tumors with a volume of 0.5 mL or less.
A recent study (Rosenkrantz AB et al,
2016) reports also moderate agreement between experienced radiologists,
which tended to be better in PZ than TZ,
although was weak for DCE in PZ.
This underscores the intrinsic robustness of the PI-RADS v2 assessment technique but also emphasises the need for specific PI-RADS v2 training,
documentation of observer variability according to reader experience,
and further data on intra- and interobserver variability.
4.2.
Lack of experience
The inappropriate use of PI-RADS v2 by new users,
without sufficient training or experience,
may be damaging.
Case conferences and multidisciplinary meetings with histopathologic correlation are helpful for calibrating the accuracy of PI-RADS category assessments.
Even if radiologists apply the system properly,
concern remains if urologists base management decisions too strictly on the assessment categories provided.
4.3.
Problematic areas
Because the dominant factors for PI-RADS v2 assessment are T2WI for the TZ and DWI for the PZ,
identification of the zonal location of the lesion is vital.
Areas in which this may be especially problematic include the interface of the CZ,
the base of the gland,
the anterior-apical region,
the interface of the anterior horn of the PZ with TZ and the anterior fibromuscular stroma.
Lesions within the anterior fibromuscular stroma and the central zone (CZ) may not be optimally evaluated using current PZ and TZ criteria.
DCE has little effect on the assessment of TZ lesions,
however,
the anterior fibromuscular stroma is usually hypovascular,
and DCE may be useful for evaluating this region.
On the other hand CZ commonly exhibits restricted diffusion and DCE may be important in the detection of tumors in the CZ.
4.4.
Criteria ambiguity
The definition of “mild-to-moderate” vs “marked” signal abnormality on high-b-value DWI is subjective,
although this differentiation is critical in determining the DWI score.
In the peripheral zone,
a lesion that is interpreted as exhibiting markedly abnormal signal intensity on the ADC map or a high-b-value image,
but not both,
does not meet the criteria for a DWI score of either 3 (“mild-to-moderate” abnormality on both image sets) or 4 (“marked” abnormality on both image sets).
This source of uncertainty can lead to variable interpretation of lesions of this nature,
and clarification is necessary.
ADC values depend on the choice of b values for DW images used for calculations (hence the recommendation to use only b values < 1000 s/mm2),
but it also depends on the diffusion time achieved on diffusion sequences (which is highly dependent on scanner specifications) and on a variety of other technical factors.
The solution would be for each institution to determine its own ADC cutoff value based on biopsy and prostatectomy results.
4.5.
Abrupt shifts
These abrupt shifts result from elevations in the assessment category that occur only at certain levels of suspicion.
For example,
a PZ lesion with DCE positive findings plus a DWI score of 2 leads to a PIRADS = 2 whereas a DWI score of 3 leads to a PIRADS = 4.
The same may happen for a TZ lesion that measures 15 mm,
with a T2WI score of 3,
which leads to a PIRADS = 3 whereas a T2WI score of 4 would lead to a PIRADS = 5.
Validation of the 1.5-cm cut-off is needed.
4.6.
False negatives
Although mpMRI is an accurate technique for detecting significant PCa,
it misses a low percentage of significant PCa (6–25%).
The missed lesions are usually invasive PCa intermixed with normal tissue,
low-grade PCa or mucinous PCa.
The rate at which this occurs is low for PI-RADS 1 and 2 lesions and higher for PI-RADS 3 lesions.
The exact prevalence of all PCa and significant PCa for each PI-RADS v2 category has yet to be determined.
Vargas HA et al report that PI-RADSv2 correctly identified 94-95 % of PCa foci ≥0.5 mL,
but was limited for the assessment of tumours ≤0.5 mL.
FAQ – What should be done when the biopsy is negative with a PI-RADS 4 or 5?
The biopsy should be repeated.
Barentsz JO et al report that there is an important PCa in 86% of PI-RADS 4 and 93% PI-RADS 5 cases.
Anterior lesions may be a problem due to the fact that the transrectal biopsy needle has a range of 20 mm which may no be sufficient to reach anterior leasions.
In the 39 sector scheme there is a line that divides the gland into anterior and posterior by the 17-mm line,
based on the likely reach of transrectal biopsy needle.
The future directions will be in the directon to continuous inprovement,
reachinga a PIRADS v3 that will probably be more objective,
including:
- ADC,
volumetry
- Include recommendations on approaching the patient
- Structured report (under development)
- PI-RADS Atlas (in development)
5.
Examples from our hospital
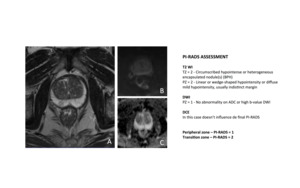
Fig. 8: 59-year-old man with prostate-specific antigen level of 6,68 ng/mL and prior negative prostate biopsy.
Axial T2-weighted MR image (A) shows circumscribed hypointense and heterogeneous nodules on transition zone, typical of benign prostate hypertrophy (BPH). The peripheral zone is hyperintense and homogeneous except for a slightly hypointense area that is not evident on DWI (B and C).
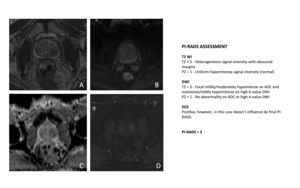
Fig. 9: 62-year-old man with elevation prostate-specific antigen and two prior negative prostate biopsies.
Axial T2-weighted MR image (A) shows approximately y-mm hypointense area of moderately decreased T2 signal within left transition zone. Lesion shows slight heterogeneity, with small foci of mildly increased T2 signal. DWI (B and C) shows corresponding moderate hyperintensity for high-b-value (B = 1400s/mm2) (B) and moderate hypointensity on ACD map (C). DCE was positive, as demonstrated with subtraction (D) but not relevant for the final PI-RADS.
Prostate biopsy revealed benign prostate hypertrophy (BPH), with no signs of malignancy.
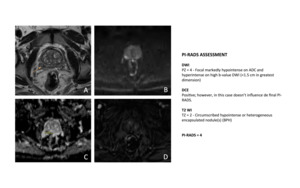
Fig. 10: 62-year-old man with elevated prostate-specific antigen level and prior negative prostate biopsy.
Axial T2-weighted MR image (A) shows focal decreased T2 signal (arrow) in right peripheral zone. DWI (B and C) showes corresponding marked hyperintensity for high-b-value (B = 1400s/mm2) (B) and marked hypointensity on ACD map (C). DCE was positive, as demonstrated with subtraction (D) but not relevant for the final PI-RADS.
Although Prostate Imaging Reporting and Data System, version 2 (PI-RADS v2), advises comparing signal of lesion on ADC map and high-b-value DW image with signal of normal tissue in same histologic zone, differentiation between mild-to-moderate and marked signal abnormality remains subjective, which in turn leads to potential variation in whether both lesion’s DWI score and overall PI-RADS assessment category is 3 or 4.
Biopsy revealed the presence of prostate adenocarcinoma Gleason score of 4 + 3.

Fig. 11: 57-year-old man with prostate-specific antigen level of 8,98 ng/mL and two prior negative prostate biopsies.
DWI shows an area in the left peripheral zone with marked hyperintensity for high-b-value (B = 1400s/mm2) (B) and marked hypointensity on ACD map (C) measuring 20 mm.
Coronal (C) and axial (D) T2-weighted MR images show an area of decreased T2 signal (arrow) that occupies most of the left lobe and extends to the right lobe (C) and with extraprostatic extension (C).
DCE was positive, as demonstrated with subtraction (E) but not relevant for the final PI-RADS.
The patient underwent a radical prostatectomy that reveled the presence of a prostate adenocarcinoma Gleason 3 + 4, in the left lobe, with extraprostatic extension, without involvement of the seminal vesicles. T3aN0.



 shows approximately y-mm hypointense area of moderately decreased T2 signal within left transition zone. Lesion shows slight heterogeneity, with small foci of mildly increased T2 signal. DWI (B and C) shows corresponding moderate hyperintensity for high-b-value (B = 1400s/mm2) (B) and moderate hypointensity on ACD map (C). DCE was positive, as demonstrated with subtraction (D) but not relevant for the final PI-RADS.
Prostate biopsy revealed benign prostate hypertrophy (BPH), with no signs of malignancy.")
 shows focal decreased T2 signal (arrow) in right peripheral zone. DWI (B and C) showes corresponding marked hyperintensity for high-b-value (B = 1400s/mm2) (B) and marked hypointensity on ACD map (C). DCE was positive, as demonstrated with subtraction (D) but not relevant for the final PI-RADS.
Although Prostate Imaging Reporting and Data System, version 2 (PI-RADS v2), advises comparing signal of lesion on ADC map and high-b-value DW image with signal of normal tissue in same histologic zone, differentiation between mild-to-moderate and marked signal abnormality remains subjective, which in turn leads to potential variation in whether both lesion’s DWI score and overall PI-RADS assessment category is 3 or 4.
Biopsy revealed the presence of prostate adenocarcinoma Gleason score of 4 + 3.")
 (B) and marked hypointensity on ACD map (C) measuring 20 mm.
Coronal (C) and axial (D) T2-weighted MR images show an area of decreased T2 signal (arrow) that occupies most of the left lobe and extends to the right lobe (C) and with extraprostatic extension (C).
DCE was positive, as demonstrated with subtraction (E) but not relevant for the final PI-RADS.
The patient underwent a radical prostatectomy that reveled the presence of a prostate adenocarcinoma Gleason 3 + 4, in the left lobe, with extraprostatic extension, without involvement of the seminal vesicles. T3aN0.")