ECR 2017 / C-1920
Imaging techniques in the diagnosis and prognosis of Multiple Myeloma: Who is our best ally?
This poster is published under an open license. Please read the disclaimer for further details.
Congress:
ECR 2017
Poster Number:
C-1920
Type:
Educational Exhibit
Keywords:
Metastases, Cancer, Blood, Diagnostic procedure, Comparative studies, MR, Digital radiography, CT, Bones
Authors:
P. Bartolomé, A. Quilez, F. M. Caballeros, L. Sancho Rodríguez, I. GONZALEZ DE LA HUEBRA RODRIGUEZ, A. Garcia Baizán, J. D. Aquerreta; Pamplona/ES
DOI:
10.1594/ecr2017/C-1920

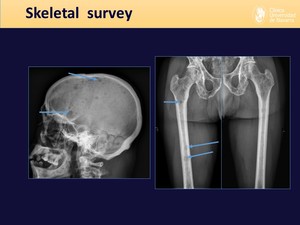
Fig. 3:
Skeletal survey: display of the 14 plain radiographs of which it's composed.
, easily detected by skeletal survey.")
Fig. 4:
Skeletal survey findings. Example of a patient with multiple lytic bone lesions...

Fig. 5:
Low sensitivity of skeletal survey. Subtle findings in the lumbar plain...

Fig. 6:
Skeletal survey: current role

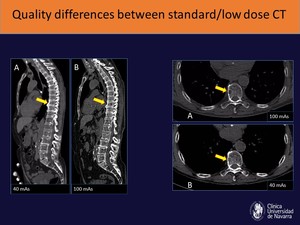
Fig. 7:
Low-dose CT allows for a precise evaluation of patients with reduced radiation...
, but clearly identifiable in the standard dose CT (100 mAs)")
Fig. 8:
In low dose studies, however, there is a reduced image quality that in most...
 in a patient with MM. Using thin-slice reconstructions, a whole body study can reach more than 1800 images, making it very time-consuming for the radiologist.")
Fig. 9:
Example of a whole body low dose CT, with multiple lytic lesions (white arrows)...

Fig. 10:
Imaging findings in whole body low dose CT studies for patients with MM.
, as opposed to the normal fatty occupation of the right humerus (-42 HU)")
Fig. 11:
Intramedullary occupation of the proximal end of the left humerus (+35 HU), as...

Fig. 12:
Example that shows the superior sensitivity of CT over skeletal survey for the...
 was only able to detect the vertebral compression fracture, whereas CT could detect multiple lytic lesions in adjacent osseous structures.")
Fig. 13:
In this case, skeletal survey (SS) was only able to detect the vertebral...

Fig. 14:
Since CT relies on bone destruction to visualize lesions, it can't detect...

Fig. 15:
Low-dose CT drawbacks

Fig. 16:
Whole body MRI standard sequences, and technical requierements for an optimal...

Fig. 17:
Diverse affectation patterns of Multiple Myeloma in MRI images.

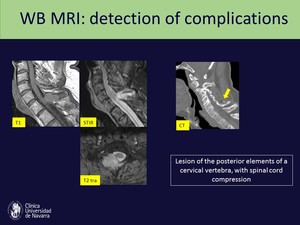
Fig. 19:
MRI ability to detect medullary complications, such as in this case, in which...

Fig. 20:
Performing a spinal + pelvic MRI is an alternative to whole body MRI with lower...

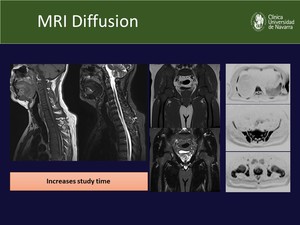
Fig. 21:
MRI conventional and diffusion-weighted sequences, with the inverted diffusion...

Fig. 22:
PET/CT overview
, more than 3 focal lesions and SUVmax value above 4.2 (39.8)")
Fig. 23:
Patient that shows all the prognostic factors associated with lower PFS and OS:...

Fig. 24:
Complete response assessed by PET. Despite the presence of a lytic lesion in...

Fig. 25:
This patient diagnosed with solitary plasmacytoma of the left knee showed an...
 criteria from the IMWG (International Myeloma Working Group) References: Shaji Kumar et al. International Myeloma Working Group consensus criteria for response and minimal residual disease assessment in multiple myeloma. The Lancet. Volume 17, No. 8, e328–e346, August 2016")
Fig. 26:
Minimal Residual Disease (MRD) criteria from the IMWG (International Myeloma...
, that represents MRD.")
Fig. 27:
Example of a patient with MM, that after treatment still presents a lesion in...

In the next study we can observe a focal increase in the metabolic activity (SUVmax: 2.8) that must not be mistaken for tumoral activity, since it represents osteoblastic reparative metabolism, identified in the CT images as an increased bony matrix.")
Fig. 28:
This patient with a plasmacytoma of the right iliac bone shower partial...

Fig. 29:
In this case we can appreciate the superior sensitivity of 11-C-MET vs 18-F-FDG...

Fig. 30:
Another example of the superiority of 11C-MET over 18F-FDG PET /CT in a patient...