The ultrasonography (US) is the primary and initial imaging modality of choice for patients presenting with right upper quadrant pain,
although there are situations where additional imaging may be required,
namely computed tomography (CT).
The most common causes of acute pain in the abdominal quadrants are listed below:
- Acute cholecystitis and its complications (gangrene cholecystitis,
emphysematous cholecystitis and gallbladder perforation)
- Choledocholithiasis
- Ascending cholangitis
- Liver abscess
- Acute pancreatitis
- Painful liver neoplasms
- Hepatic artery aneurysm
- Budd-chiari syndrome
- Perforated duodenal ulcer
- Gallstone ileus
- Intraperitoneal focal fat infarction
- Ascending Retrocecal Appendicitis
1. ACUTE CHOLECYSTITIS AND ITS COMPLICATIONS
Acute cholecystitis is a primary diagnostic consideration in patients presenting with acute right upper quadrant pain.
Classically,
these patients experience an acute pain that increases in intensity over several minutes and then persists for several hours.
It can be accompanied by nausea,
vomiting,
anorexia and fever.
The physical examination is presented with murphy´s sign.
Most cases of acute cholecystitis are acute calculous cholecystitis.
About 95% of these cases are related due to calculous obstruction of the gallbladder neck or cystic duct.
However,
the cholecystitis can be acalculous,
in critically ill or injured patients,
by conditions that can promote ischaemia injury to the gallbladder,
such as: major surgery,
serious trauma,
mechanical ventilation,
extensive burns,
or prolonged parenteral nutrition.
IMAGING FINDINGS:
The ultrasound has an important and fundamental role in the diagnosis of acute cholecystitis.
The presence of gallstones in combination with maximal tenderness over the gallbladder has a high degree of prediction.
Other signs less sensitivity and specificity can be seen,
such as gallbladder wall edema and thickening,
pericholecystic fluid and distended gallbladder.

Fig. 1: Acute cholecystitis – Distended gallbladder filled with echogenic sludge and gallstones. The gallbladder wall is markedly thickened with presence of pericholecystic fluid (arrows).
References: Radiology Department, Coimbra University Hospital - Coimbra/PT

Fig. 2: Acute cholecystitis - The gallbladder is filled with echogenic sludge and gallstones. The wall is markedly thickened and there is pericholecystic fluid (arrows).
References: Radiology Department, Coimbra University Hospital - Coimbra/PT
1.1 Gangrenous Cholecystitis
Gangrenous cholecystitis is a rare and severe complication of acute cholecystitis.
The increased intraluminal pressure may produce gallbladder wall ischemia following by necrosis.
The murphy sign is only present in 33% of patients,
maybe because of damage to the gallbladder wall innervation by gangrenous changes.
These patients have a high risk of perforation,
and must be treated as soon as possible.
IMAGING FINDINGS:
In ultrasound assessment,
it is traduced by alternating hyperechoic and hypoechoic bands in an irregularly thickened gallbladder wall,
traducing intraluminal membranes. At CT is seen gas in the wall or lumen,
intraluminal membranes,
irregular or absent wall and abscess.

Fig. 3: Gangrenous Cholecystitis - Irregularly thickened gallbladder wall, with hypoechoic intraparietal areas compatible with a process of necrosis (arrowheads). There are a calculus and sludge inside the gallbladder.
References: Radiology Department, Coimbra University Hospital - Coimbra/PT
1.2 Emphysematous Cholecystitis
Emphysematous cholecystitis is characterized by the presence of intramural and/or intraluminal gas.
The disease begins with acute cholecystitis followed by ischemia or gangrene of the gallbladder wall and an infection caused by gas-producing bacteria (commonly Clostridium perfringens,
Escherichia coli and Bacterioides fragilis).This condition has a significantly increased rates of mortality (15-25%) and it is considered a surgical emergency.
IMAGING FINDINGS:
The imaging findings have an important diagnostic value in this cases.
The conventional radiography may show air in the wall or lumen of the gallbladder with presence of air-fluid levels.
The ultrasonography may demonstrate highly echogenic reflectors with low-level posterior shadowing and reverberation artifact.
In some cases,
can be performing CT to a best evaluation,
since it is the most sensitive and specific imaging modality in the diagnosis of emphysematous cholecystitis.

Fig. 4: Emphysematous cholecystitis - The conventional radiography shows gas in the right hypochondrium (arrows), compatible with air in the gallbladder wall. The level air-fluid seen adjacent to the gallbladder is related with "sentinel loop". The ultrasonography demonstrates a distended gallbladder with thickened wall and a calculus in the infundibulum. There are highly echogenic reflectors with low-level posterior shadowing and reverberation artefact (arrowhead).
References: Radiology Department, Coimbra University Hospital - Coimbra/PT

Fig. 5: Emphysematous cholecystitis – Computed Tomography shows signs of cholecystitis (gallbladder distention, wall thickening, pericholecystic fat stranding) with presence of gas in the wall and lumen (arrowhead).
References: Radiology Department, Coimbra University Hospital - Coimbra/PT
1.3 Gallbladder Perforation
Gallbladder perforation is a serious complication of acute cholecystitis and carry a relatively high mortality rate.
It complicates acute cholecystitis in up to 10% of cases.
Niemeier classified gallbladder perforations in three categories: acute free perforation with generalized peritonitis (type I) ; subacute pericholecystic abscess (type II) ; chronic cholecystoenteric fistulation (type III).
Subacute perforations are the most common,
accounting for 60% of all cases.
The cholecystoduodenal fistula is the most common chronic perforation and can be following by pneumobilia.
IMAGING FINDINGS:
Ultrasound and CT scans are reliable tools for diagnosing gallbladder perforations by identifying the defect in the wall,
despite CT is more accurately to demonstrate the fistulas.

Fig. 6: Gallbladder perforation type II – We can see two clinic cases (A and B) of acute cholecystitis complicated with wall perforation, with illustration of the focal wall defect (arrows) and pericholecystic abscess (arrowheads).
References: Radiology Department, Coimbra University Hospital - Coimbra/PT
2. Choledocholithiasis
Choledocholithiasis is the presence of a gallstone in the common bile duct.
When a stone becomes lodged in the duct and obstructs it,
the patient may experience acute right upper quadrant and/or jaundice.
IMAGING FINDINGS:
The diagnosis is performed initially by ultrasound that has relatively higher sensibility in the detection of choledocholithiasis.
Ultrasound should be performed both proximal and distal common bile duct individually,
in longitudinal and transverse planes.
If choledocholithiasis is suspected but cannot be confirmed with US,
MR cholangiopancreatography is an excellent choice for further investigations,
with high sensibility and specificity (approaching 100%).
It is the gold standard for the diagnosis of choledocholithiasis.
Another alternative is computed tomography.

Fig. 7: Choledocholithiasis - We can see two clinic cases of gallstones in the common bile duct causing obstruction and bile duct dilatation.
References: Radiology Department, Coimbra University Hospital - Coimbra/PT
3. Ascending Cholangitis
Ascending cholangitis is an infection of the bile duct,
usually caused by bacteria ascending from its junction with the intestine.
It tends to occur in an obstructed biliary system,
most commonly due to bile duct stones.
Patients with cholangitis are febrile,
often have abdominal pain,
and are jaundiced (Charcot triad).
IMAGING FINDINGS:
Noninvasive diagnostic techniques include sonography,
which is the recommended initial imaging modality. On ultrasound we should see thickening of the walls of the bile ducts and biliary dilatation with stones and/or echogenic content within the common bile duct.
CT can be important to confirm the cause of biliary obstruction,
but others findings of cholangitis are non-specific and should be interpreted in the correct clinical context.

Fig. 8: Ascending Cholangitis - Ultrasonography illustrates thickening of the bile ducts walls and biliary dilatation.
References: Radiology Department, Coimbra University Hospital - Coimbra/PT

Fig. 9: Ascending Cholangitis - CT scan shows dilatation of the intrahepatic bile ducts with parietal thickening (arrows) and heterogeneous content. There is aerobilia.
References: Radiology Department, Coimbra University Hospital - Coimbra/PT
4. Liver Abscess
Hepatic abscess is a circumscribed,
often encapsulated and purulent inflammation with necrosis of the local parenchyma caused by a multitude of pathogens (most of them are anaerobic).
Patients with liver abscess usually present with fever and right upper quadrant pain.
Others less common symptoms are jaundice,
anorexia or weight loss.
IMAGING FINDINGS:
The sonographic appearances are varied.
Usually is a low echoic to mixed-echoic lesion and the margin may be blurred or irregular due to inflammation of surrounding areas.
There may be internal septations or stranding.
Gas bubbles may also be seen.
Color Doppler will demonstrate absence of central perfusion.
Sometimes hepatic abscess can have a most solid sonographic appearance and,
mainly in this cases,
CT may complement ultrasonography by demonstrating areas of liquefaction.

Fig. 10: Liver abscess – We can see two cases of pyogenic liver abscesses with hypoechoic solid appearance.
References: Radiology Department, Coimbra University Hospital - Coimbra/PT

Fig. 11: Liver abscesses. A) Contrast-enhanced CT shows a pyogenic abscess. Grouping of low attenuation lesions in the liver - cluster sign; B) Contrast-enhanced CT shows a klebsiella abscess in the right liver lobe. Discontinuous septa (white arrow) – septal breakage sign; C) Contrast-enhanced CT shows a amoebic abscess. Thick enhancing wall and outer hypodense rim - Double target sign (black arrow).
References: Radiology Department, Coimbra University Hospital - Coimbra/PT
5. Acute Pancreatitis
Acute pancreatitis is an acute inflammation of the pancreas.The most common cause is gallstones that can lodge in the common bile duct and block the pancreatic duct.
The diagnosis is usually made by the presence of acute onset of persistent,
severe upper abdomen pain (most often located in the epigastric) and lipase/amylase elevation three times upper the limit of normal.
Diagnostic imaging may be obtained when the clinic diagnosis is in doubt,
when pancreatitis is severe,
or when a given study might provide specific information required.
IMAGING FINDINGS:
Acute pancreatitis manifests with interstitial edema and an enlarged hypoechoic gland on ultrasound.
It is also useful to the detection of cholelithiasis and choledocholithiasis and identification of peripancreatic acute fluid collections.
Contrast-enhanced CT can be important to evaluate the pancreatic morphology and viability.
Nonenhancement of all or part of the gland is termed “necrosis”.
CT is 100% specific for necrosis if greater than 30% of the gland is nonenhancing.

Fig. 12: Acute pancreatitis - Interstitial edema and an enlarged hypoechoic gland.
References: Radiology Department, Coimbra University Hospital - Coimbra/PT

Fig. 13: Acute pancreatitis – Axial contrast-enhanced CT scan shows an enlarged pancreas and small focus of non-enhancing (arrow), indicative of parenchymal necrosis. There is a small amount of peripancreatic fluid collection (arrowheads) and fat infiltration.
References: Radiology Department, Coimbra University Hospital - Coimbra/PT
6. Painful Liver Neoplasms
A liver mass can develop acute pain in result of some complications as rupture or hemorrhage.
In this context,
one of the most important liver mass is the hepatic adenoma.
Hepatic adenoma is a rare benign liver tumor associated with women that using oral contraceptive pills,
anabolic steroids and type 1 glycogen storage disease (or Von Gierke disease).
IMAGING FINDINGS
On ultrasound,
the hepatic adenoma may appear as a well-demarcated heterogeneous mass with a variable echogenicity and a hypoechoic halo of focal fat sparing.
On CT may appear as a well marginated lesion and isoattenuating to liver.
On contrast administration,
they demonstrate transient relatively homogenous enhancement returning to near isodensity on portal venous and delayed phase image.
The presence of a heterogeneous liver mass with internal hemorrhage and/or hemoperitoneum is suggestive of spontaneous rupture or hemorrhage.

Fig. 14: Rupture and hemorrhage of a hepatic adenoma – (a) Non-Contrast-Enhanced CT – heterogenous liver mass with spontaneously hyperdense areas; (b) Contrast-Enhanced CT – the tumor shows minimal heterogeneous enhancement, inferior to the liver parenchyma; (c) Non-Contrast-Enhanced CT – In the pelvis there is a moderate amount of spontaneously hyperdense fluid – hemorrhagic.
References: Radiology Department, Coimbra University Hospital - Coimbra/PT
Others neoplasms can development acute pain in the right upper quadrant as a result from rupture or hemorrhage: hepatocellular carcinoma,
its estimated rupture and spontaneous hemorrhage occurs in up to 10% of cases; cavernous hemangiomas,
its rupture and hemorrhage is very rare; vascular liver metastases,
for example from renal cell carcinoma and neuroendocrine tumors.
7. Hepatic Artery Aneurysm
Hepatic artery aneurysms are rare lesions (20% of all visceral aneurysms) and difficult to diagnose clinically.
Nevertheless,
it can be present as right upper quadrant pain,
obstructive jaundice,
or rarely as bleeding into the gastrointestinal tract.
IMAGING FINDINGS:
US is an excellent noninvasive method in detection of hepatic artery aneurism.
Spectral Doppler can aid in differentiating vascular from other types of masses and color Doppler shows arterial or turbulent flow in the lesion suggestive of it being a mass of vascular origin.
The CT angiography is useful for detecting aneurysms and assessing anatomical details,
and is being used instead of angiography.

Fig. 15: Hepatic artery aneurysm – CT scan after intravenous contrast clearly demonstrates the lumen of the hepatic artery aneurysm (arrow).
References: Radiology Department, Coimbra University Hospital - Coimbra/PT
8. Budd-Chiairi Syndrome
Budd–Chiari syndrome is a very rare condition.
The condition is caused by hepatic venous outflow obstruction at any level from the small hepatic veins to the junction of the inferior vena cava and the right atrium.
There are many causes of obstruction,
including thrombosis of the hepatic vein and compression of the hepatic vein by an outside structure (e.g.
tumor).
Usually it presents with the classical triad of abdominal pain,
ascites and hepatomegaly,
although this is non-specific presentation.
IMAGING FINDINGS:
The imaging findings of Budd-Chiari syndrome are variable and depend on the stage of the disease.
In the acute stage,
usually ultrasound can show hepatomegaly,
splenomegaly,
heterogeneous echotexture and ascites.
Duplex Doppler ultrasonography (US) shows absent or flat flow in the hepatic veins,
reversed flow in the hepatic veins,
inferior vena cava or both,
and intrahepatic collateral pathways.
At the level of the portal vein,
reveals slow hepatofugal flow (< 11 cm/s).
Computed tomography reveals a decreased peripheral hepatic enhancement caused by portal and sinusoidal stasis and stronger enhancement of the central portion of the liver parenchyma.
The caudate lobe is enlarged and demonstrates increased contrast enhancement compared with the remainder of the liver.

Fig. 16: Budd-Chiairi Syndrome - Contrast- enhanced CT depicts a moderately enlarged liver with characteristic patchy enhancement and sparing of the caudate lobe (white asterisk), and also a small amount of peritoneal fluid (more evident in b).
References: Radiology Department, Coimbra University Hospital - Coimbra/PT
9. Perforated Duodenal Ulcer
Perforation complicates duodenal ulcer about half as often as bleeding and most perforated ulcers are on the anterior surface of the duodenum.
The first and most characteristic symptom is an intense and severe epigastric pain that rapidly becomes generalized.
The abdominal findings are characteristically described as of board-like rigidity.
IMAGING FINDINGS:
As an initial evaluation,
the radiography can show the presence of gas within peritoneal cavity.
CT is the following modality of choice in this situation.
The signs of duodenal perforation include extraluminal air,
pneumoperitoneum,
duodenal wall thickening,
periduodenal fat stranding,
discontinuity of the duodenal wall,
air bubbles in close proximity to the site of perforation,
extravasation of oral contrast material and abscess.

Fig. 17: Perforated Duodenal Ulcer – a) CT shows the location of the duodenal ulcer perforation (white arrow), with gas accumulation and positive oral contrast in the right anterior pararenal space (black asterisk); b) Endoscopy reveals wide and deep necrotic ulceration in the posterior wall of the duodenal bulb.
References: Radiology and Gastroenterology Departments, Coimbra University Hospital - Coimbra/PT. Courtesy of J. Brito, Portimão/PT
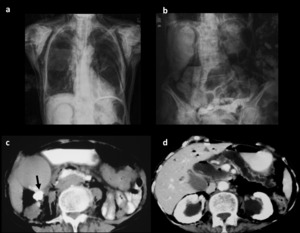
Fig. 18: Duodenal perforation after endoscopic retrograde cholangiopancreatography (ERCP) - a and b) Radiographs of the chest and abdomen show extensive collections of gas, with pneumoretroperitoneum and pneumomediastinum, as well as subcutaneous and cervical emphysema; c and d) CT with positive hydrosoluble oral contrast shows retroperitoneal extravasation to the right anterior pararenal space (arrow) with abundant retroperitoneal gas. The gallbladder is distended with presence of gallstones. There are gas in the intrahepatic bile ducts and dilatation of the main pancreatic duct with marked atrophy of the pancreatic parenchyma.
References: Radiology Department, Coimbra University Hospital - Coimbra/PT. Courtesy of J. Brito, Portimão/PT
10. Gallstone Ileus
Gallstone Ileus is an uncommon cause of mechanical small bowel obstruction.
It occurs when gallstones impact in the lumen of the bowel.
The stone enters the gastrointestinal tract usually through a cholecystenteric fistula located between the gallbladder and the duodenum.
Gallstone ileus can acutely present as colicky abdominal pain and abdominal distension in the course of small bowel obstruction.
IMAGINNG FINDINGS:
Classically the findings on abdominal radiographs are a small bowel obstruction,
gas within the biliary tree and a ectopic gallstone on abdominal plain radiograph - Rigler´s triad. CT is very helpful in diagnosing of lithiasis,
although it depends of the quantity of calcification.
In these situations,
ultrasound can be useful,
because gallstone always appears as a hyperechoic mass with distal acoustic shadowing.

Fig. 19: Gallstone Ileus - a) Radiograph of the abdomen reveals an air-fluid level in the gallbladder (arrow) and a calculus (arrowhead); b and c) CT scan shows air-fluid level in gallbladder (asterisk) and diffuse thickening of the duodenal wall (arrow); d) There is a calculus in the small bowel (arrow).
References: Radiology Department, Coimbra University Hospital - Coimbra/PT
11. Intraperitoneal Focal Fat Infarction
The term intraperitoneal focal fat infarction (IFFI) includes a variety of acute abdominal clinical conditions with focal fatty tissue necrosis.
In clinical practice,
most cases of IFFI include torsion and/or infarction of the greater omentum or of the epiploic appendages.
Epiploic appendagitis is an uncommon cause of abdominal pain.
The greatest concentration of epiploic appendages is in the cecum and sigmoid colon.
Involvement of the proximal colon is less common,
although not unusual.
IMAGING FINDINGS:
The characteristics of acute epiploic appendagitis on US images are an oval noncompressible hyperechoic mass at the site of maximum tenderness,
adjacent to the colon,
with no central blood flow depicted on color Doppler US images.The most common CT feature is an oval fat-density lesion less than 5 cm in diameter with surrounding inflammatory changes abutting the anterior colonic wall.
Thickening of the parietal peritoneum,
secondary to the spread of inflammation,
also may be observed.
The presence of a central area of high attenuation within the fat (due to venous thrombosis) is useful for the diagnosis.

Fig. 20: Epiploic appendagitis - CT scan illustrates a rounded mass adjacent to the ascending colon (arrows) displaying a central density of fat and a denser peripheral rim.
References: Radiology Department, Coimbra University Hospital - Coimbra/PT
Omental infarction is a rare cause of acute abdomen resulting from vascular compromise of the greater omentum. The right inferior portion of the omentum is more vulnerable to infarction due to a more tenuous blood supply.
However,
it can occur along of all portions of the omentum.
IMAGING FINDINGS:
Ultrasonography shows a focal area of increased echogenicity in the omental fat.
On CT,
classically it appears as a fatty and large (>5 cm) encapsulated mass,
with hyperdense peripheral halo and soft-tissue stranding adjacent to the ascending colon.

Fig. 21: Omental Infarction - Ultrasonography show a focal area of increased echogenicity in the omental fat (arrows)
References: Radiology Department, Coimbra University Hospital - Coimbra/PT

Fig. 22: Omental infarction - CT scan illustrates a fatty and large (>5 cm) mass (arrow) associated with soft-tissue stranding in the greater omentum, anterior to the ascending colon.
References: Radiology Department, Coimbra University Hospital - Coimbra/PT
12.
Ascending Retrocecal Appendicitis
Acute appendicitis is the most common cause of acute abdominal pain in adults.
However,
some patients may have atypical presentation related to the position of the appendix that may lead to a delay in diagnosis and increased complications.
Most of the patients with ascending subhepatic retrocecal appendicitis may experience right upper abdominal pain.
It may give rise to an abscess in the subhepatic space and spread to the tail of the liver,
or it may spread along the right paracolic gutter,
and extend to the right subphrenic spaces.
IMAGING FINDINGS:
Ultrasound is used frequently in the assessment of suspected acute appendicitis in young children and sometimes in adults,
but it requires expertise,
and dedicated techniques using graded compression to expose the appendix and displace surrounding bowel loops.
However,
in adults,
un-enhanced CT has been shown to be more sensitive in diagnosing acute appendicitis than ultrasound is.
CT is very sensitive for evaluating the normal and thickened wall appendix,
inflamed peri-appendiceal fat,
collections,
and presence of free gas in ruptured appendix.
Signs of appendicitis are a thickened appendiceal wall above 2 mm with ringlike contrast enhancement,
a cross-sectional diameter above 6 mm,
periappendiceal fat attenuation,
a calcified appendicolith,
and abscess formation.
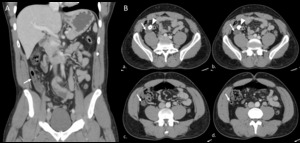
Fig. 23: Ascending retrocecal appendicitis – Contrast-enhanced CT – A. Coronal reconstruction shows the long thickened and inflamed ascending retrocecal appendix (arrow) reaching the subhepatic region with inflammatory stranding; B (a-d). Ascending cross sections of the abdomen show thickened ascending retrocecal appendix (arrow) with mild inflammatory changes and presence of a calcified appendicolith in the appendix (arrowhead).
References: Radiology Department, Coimbra University Hospital - Coimbra/PT

Fig. 24: Ascending retrocecal appendicitis – Contrast-enhanced CT – A. Coronal reconstruction shows the long ascending retrocecal appendix (arrow) reaching the subhepatic region and a fluid collection in the right lateral paracolic gutter extending superiorly to the subhepatic region (asterisk) with inflammatory stranding; B (a-d). Ascending cross sections of the abdomen show long ascending retrocecal appendix (arrows), with stranding of the surrounding fat and fluid collection in the subhepatic region (arrowhead), surrounding the tip of the right liver lobe.
References: Radiology Department, Coimbra University Hospital - Coimbra/PT

. References: Radiology Department, Coimbra University Hospital - Coimbra/PT")
. References: Radiology Department, Coimbra University Hospital - Coimbra/PT")
. There are a calculus and sludge inside the gallbladder. References: Radiology Department, Coimbra University Hospital - Coimbra/PT")
, compatible with air in the gallbladder wall. The level air-fluid seen adjacent to the gallbladder is related with "sentinel loop". The ultrasonography demonstrates a distended gallbladder with thickened wall and a calculus in the infundibulum. There are highly echogenic reflectors with low-level posterior shadowing and reverberation artefact (arrowhead). References: Radiology Department, Coimbra University Hospital - Coimbra/PT")
 with presence of gas in the wall and lumen (arrowhead). References: Radiology Department, Coimbra University Hospital - Coimbra/PT")
 of acute cholecystitis complicated with wall perforation, with illustration of the focal wall defect (arrows) and pericholecystic abscess (arrowheads). References: Radiology Department, Coimbra University Hospital - Coimbra/PT")


 and heterogeneous content. There is aerobilia. References: Radiology Department, Coimbra University Hospital - Coimbra/PT")

 Contrast-enhanced CT shows a pyogenic abscess. Grouping of low attenuation lesions in the liver - cluster sign; B) Contrast-enhanced CT shows a klebsiella abscess in the right liver lobe. Discontinuous septa (white arrow) – septal breakage sign; C) Contrast-enhanced CT shows a amoebic abscess. Thick enhancing wall and outer hypodense rim - Double target sign (black arrow). References: Radiology Department, Coimbra University Hospital - Coimbra/PT")

, indicative of parenchymal necrosis. There is a small amount of peripancreatic fluid collection (arrowheads) and fat infiltration. References: Radiology Department, Coimbra University Hospital - Coimbra/PT")
 Non-Contrast-Enhanced CT – heterogenous liver mass with spontaneously hyperdense areas; (b) Contrast-Enhanced CT – the tumor shows minimal heterogeneous enhancement, inferior to the liver parenchyma; (c) Non-Contrast-Enhanced CT – In the pelvis there is a moderate amount of spontaneously hyperdense fluid – hemorrhagic. References: Radiology Department, Coimbra University Hospital - Coimbra/PT")
. References: Radiology Department, Coimbra University Hospital - Coimbra/PT")
, and also a small amount of peritoneal fluid (more evident in b). References: Radiology Department, Coimbra University Hospital - Coimbra/PT")
 CT shows the location of the duodenal ulcer perforation (white arrow), with gas accumulation and positive oral contrast in the right anterior pararenal space (black asterisk); b) Endoscopy reveals wide and deep necrotic ulceration in the posterior wall of the duodenal bulb. References: Radiology and Gastroenterology Departments, Coimbra University Hospital - Coimbra/PT. Courtesy of J. Brito, Portimão/PT")
 - a and b) Radiographs of the chest and abdomen show extensive collections of gas, with pneumoretroperitoneum and pneumomediastinum, as well as subcutaneous and cervical emphysema; c and d) CT with positive hydrosoluble oral contrast shows retroperitoneal extravasation to the right anterior pararenal space (arrow) with abundant retroperitoneal gas. The gallbladder is distended with presence of gallstones. There are gas in the intrahepatic bile ducts and dilatation of the main pancreatic duct with marked atrophy of the pancreatic parenchyma. References: Radiology Department, Coimbra University Hospital - Coimbra/PT. Courtesy of J. Brito, Portimão/PT")
 Radiograph of the abdomen reveals an air-fluid level in the gallbladder (arrow) and a calculus (arrowhead); b and c) CT scan shows air-fluid level in gallbladder (asterisk) and diffuse thickening of the duodenal wall (arrow); d) There is a calculus in the small bowel (arrow). References: Radiology Department, Coimbra University Hospital - Coimbra/PT")
 displaying a central density of fat and a denser peripheral rim. References: Radiology Department, Coimbra University Hospital - Coimbra/PT")
 References: Radiology Department, Coimbra University Hospital - Coimbra/PT")
 mass (arrow) associated with soft-tissue stranding in the greater omentum, anterior to the ascending colon. References: Radiology Department, Coimbra University Hospital - Coimbra/PT")
 reaching the subhepatic region with inflammatory stranding; B (a-d). Ascending cross sections of the abdomen show thickened ascending retrocecal appendix (arrow) with mild inflammatory changes and presence of a calcified appendicolith in the appendix (arrowhead). References: Radiology Department, Coimbra University Hospital - Coimbra/PT")
 reaching the subhepatic region and a fluid collection in the right lateral paracolic gutter extending superiorly to the subhepatic region (asterisk) with inflammatory stranding; B (a-d). Ascending cross sections of the abdomen show long ascending retrocecal appendix (arrows), with stranding of the surrounding fat and fluid collection in the subhepatic region (arrowhead), surrounding the tip of the right liver lobe. References: Radiology Department, Coimbra University Hospital - Coimbra/PT")