ECR 2017 / C-2490

Functional disorders of the ano-rectal compartment – the diagnostic role of dynamic MRI
This poster is published under an open license. Please read the disclaimer for further details.
Congress:
ECR 2017
Poster Number:
C-2490
Type:
Educational Exhibit
Keywords:
Pelvis, Gastrointestinal tract, MR, Imaging sequences, Pelvic floor dysfunction
Authors:
A. P. Caetano, D. Sofia, E. Alves; Lisbon/PT
DOI:
10.1594/ecr2017/C-2490

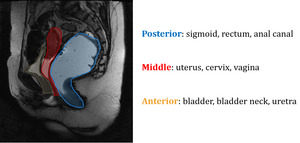
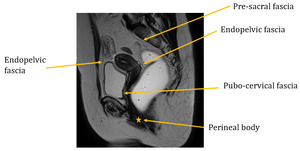
Fig. 1:
Sagital slice showing the pelvic compartments
 Atlas of human anatomy. Saunders, 6th edition. References: Netter FH. (2014) Atlas of human anatomy. Saunders, 6th edition")
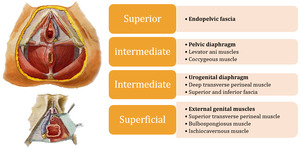
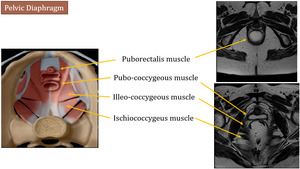
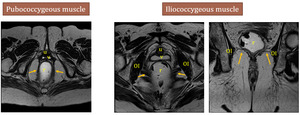
Fig. 2:
Left images are adapted from - Netter FH. (2014) Atlas of human anatomy....

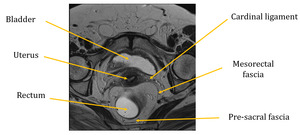
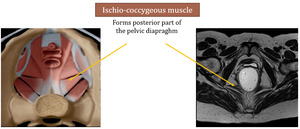
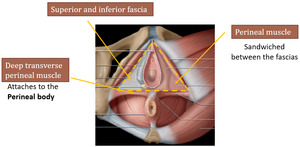
Fig. 3

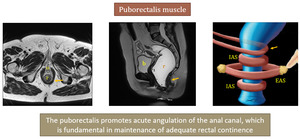
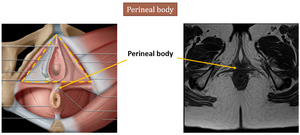
Fig. 4
 References: Shaaban AM, et al. (2015) Diagnostic Imaging gynecology. Elsevier")
Fig. 5:
Left image is adapted from Shaaban AM, et al. Diagnostic Imaging gynecology....
 References: Shaaban AM, et al. Diagnostic Imaging gynecology. Elsevier (2015)")
Fig. 6:
Left image is adapted from Shaaban AM, et al. Diagnostic Imaging gynecology....
 References: Shaaban AM, et al. Diagnostic Imaging gynecology. Elsevier (2015)")
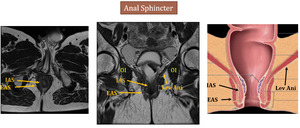
Fig. 7:
b - bladder, r - rectum, u - urethra, IAS - internal anal sphincter, EAS -...

Fig. 12:
Measurement lines - summary

Fig. 13:
Pubo-coccygeal line

Fig. 14:
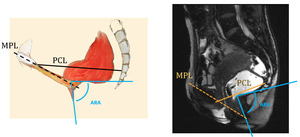
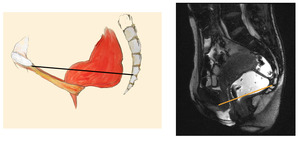
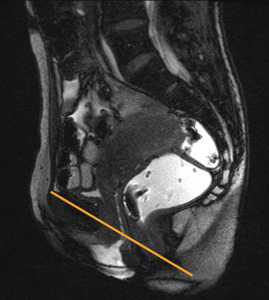
Mid-pubic line

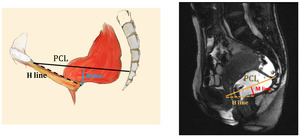
Fig. 15:
M-line and H-line, relative to the PCL

Fig. 16:
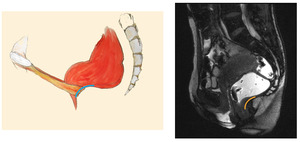
Ano-rectal junction

Fig. 17:
Ano-rectal junction

Fig. 18:
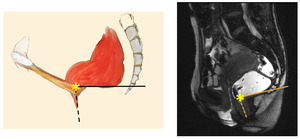
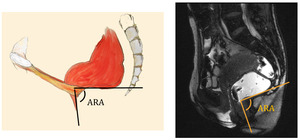
Ano-rectal angle

Fig. 19

Fig. 20:
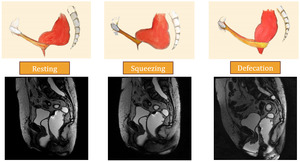
MRI dynamic evaluation of defecation

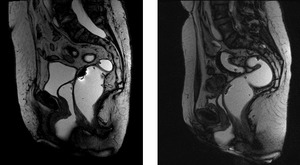
Fig. 21:
Resting - normal MRI sagital images

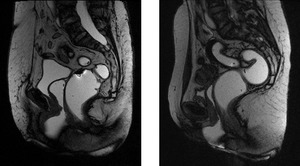
Fig. 22:
Squeezing - normal MRI sagital images

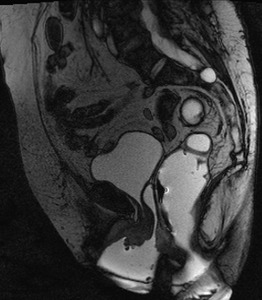
Fig. 23:
Defecation - normal MRI sagital image

Fig. 24

Fig. 25:
Arrows - rectal intussusception
Left image - schematics of rectal...

Fig. 26

Fig. 27

Fig. 28

Fig. 29

Fig. 30

Fig. 31