This paper will give a detailed review on the anatomy of the pterygopalatine fossa (PPF),
which can be considered a major crossroad of multiple head and neck neurovascular structures.
Knowledge of this anatomy is of great importance in disease spreading along the nerves connected to the PPF.
We'll present some cases of pathology involving the PPF.
The direct and indirect radiological signs of perineural spread will be discussed in this exhibition.
A.
ANATOMY OF THE PTERYGOPALATINE FOSSA
The pterygopalatine fossa is a fat-containing inverted pyramid-shaped space,
which is bounded by the posterior wall of the maxillary sinus,
pterygoid process and perpendicular plate of the palatine bone.
As a general,
obliteration of this normal fat should alert the radiologist to search for pathology.
Overview of connections to the PPF:
| Anatomical structure |
Canal |
Position in the PPF
|
| Palate |
Greater and lesser palatine canals |
Inferior |
| Palate |
palatovaginal or pharyngeal canal (inconsistently seen on imaging) |
Inferoposterior |
| Middle cranial fossa |
Vidian or pterygoid canal |
Inferoposterior |
| Nasal cavity |
Sphenopalatine foramen |
Medial |
| Infratemporal fossa |
Pterygomaxillary fissure |
Lateral |
| Orbit |
Inferior orbital fissure |
Anterior |
| Middle cranial fossa |
Foramen rotundum |
Superoposterior |
A.1.
Greater and lesser palatine canal
The most caudal opening of the PPF is the greater palatine canal (apex of the inverted pyramid) descending in the posteroinferior aspect of the medial wall of the maxillary bone.
It ends in the posterolateral aspect of the hard palate as the greater palatine foramen (GPF).
The lesser palatine canal can be found posterior to the greater palatine canal traversing the pyramidal process of the palatine bone.
It ends in its inferior aspect as the lesser palatine foramen.
The canals house the lesser and greater palatine nerves.
Both can be consistently seen on axial CT imaging and thin section coronal images.
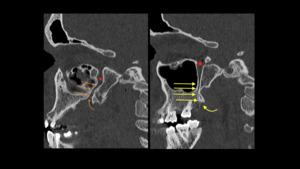
Fig. 1: Sagital HRCT shows the greater (orange arrow) and lesser (yellow arrow) palatine canal with respectively the greater palatine foramen (orange curved arrow) and lesser palatine foramen (yellow curved arrow). PPF (red star).
References: Gert-Jan Allemeersch, Department of Radiology, UZ Brussel - Brussels/BE
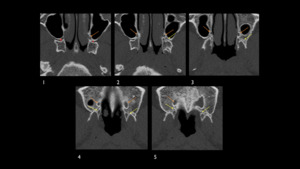
Fig. 2: Axial HRCT shows the greater (orange arrow) and lesser (yellow arrow) palatine canal from the PPF (red star) cranial to caudal (1-5).
References: Gert-Jan Allemeersch, Department of Radiology, UZ Brussel - Brussels/BE
A.2.
Pterygomaxillary fissure
The pterygomaxillary fissure connects the lateral PPF with the infratemporal fossa and transmits the terminal part of the maxillary artery and the posterior superior alveolar nerve.
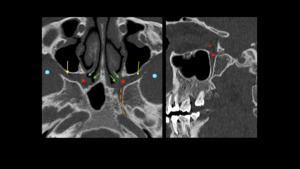
Fig. 3: Axial and sagital HRCT of the PPF (red star) at the level of the Vidian canal. Communication on the lateral side with the infratemporal fossa (blue dot) via the pterygomaxillary fissure (yellow arrow) and on the medial side with the nasal cavity via the sphenopalatine foramen (green arrows).
The PPF communicates with the foramen lacerum via the Vidian canal (orange stripes).
Communication with the orbit via the infraorbital fisseure (red arrow).
References: Gert-Jan Allemeersch, Department of Radiology, UZ Brussel - Brussels/BE
A.3.
Palatovaginal or pharyngeal canal
The palatovaginal canal is a short bone tunnel that extends from the pterygopalatine fossa to the roof of the pharynx.
It is found inferomedially of the posterior wall of the pterygopalatine fossa,
in the roof of the nasopharynx.
It contains the pharyngeal artery and the pharyngeal nerve.
A.4.
Vidian/pterygoid canal
The roof of the PPF is formed by the sphenoid bone.
Posterolaterally through the body of the sphenoid bone traverses the Vidian canal (Fig. 3) which communicates with the foramen lacaerum and the carotid canal.
The Vidian canal contains the Vidian nerve or nervus pterygoideus.
It carries PS preganglionic nerves from the Facial nerve to the PPG.
A.5.
Sphenopalatine foramen
At the same level of the Vidian canal the PPF communicates withe the nasal cavity via the sphenopalatine foramen (Fig.
6) which is anterior to the Vidian canal opening.
The sphenopalatine foramen transmits the sphenopalatine artery and the posterior superior nasal nerves.
A.6.
Inferior orbital fissure
At the most cranial part of the inverted pyramid,
the PPF communicates with the orbit via the inferior orbital fissure ( Fig. 3,
Fig. 4 )which transmits the zygomatic branch of V2,
ascending branches from the PPG and the infraorbital nerve.

Fig. 4: Coronal HRCT of the PPF at the level of the infraorbital fossa (blue dot). Communication of the PPF (red star) with the infratemporal fossa (blue dot) via the pterygomaxillary fissure (yellow arrow). Communication of the PPF (redstar) with the nasal cavity via the sphenopalatine forman (green arrows) on the medial side. Communication with the orbital apex via the infraorbital fissure (red arrows).
References: Gert-Jan Allemeersch, Department of Radiology, UZ Brussel - Brussels/BE
A.7.
Foramen rotundum
At the same level of the inferior orbital fissure,
the middle cranial fossa communicates with the PPF via the foramen rotundum at its posterosuperior aspect.
It contains the V2 nerve that enters the PPF and continues as the infraorbital nerve.

Fig. 5: Axial HRCT shows the PPF (red star) communicating with the middle cranial fossa (yellow star) at the level of the foramen rotundum (green arrow).
References: Gert-Jan Allemeersch, Department of Radiology, UZ Brussel - Brussels/BE
B.
PERINEURAL SPREAD (PNS) IN HEAD AND NECK PATHOLOGY
Since the PPF is a crossing of many nerves,
perineural spread via direct or indirect tumoural invasion is a common finding.
The radiologist must be aware of this entity and search for pathology in the different connections from the PPF.
Presence of PNS in the PPF and its communications has important treatment and prognostic implications.
PNS has negative percussions on treatment,
because if present it requires larger radiation fields or more extensive surgical resection.
It also has important prognostic implications since PNS tends to be an independent indicator of poor prognosis in the TNM classification.
It is also considered with increased local recurrence.
The nerves frequently associated with PNS are the cranial nerves V and VII ,
since they have the largest regional spread.
Since the PPF is a central station in the trigeminal nerve pathway,
it is often the site of PNS,
typically from cancers of the cheek,
palate,
maxillary sinus and nasopharynx.
PNS is often seen in adenoid cystic carcinoma (ACC) and in a minority of nasopharyngeal carcinoma (NPC),
which is a more frequent tumour than ACC.
ACC is a form of adenocarcinoma that begins in glandular tissues and is mainly found in minor or major salivary glands.
NPC id the most common primary tumor in the nasopharynx.
It's a very agressive tumor of squamous cells that often spreads out of the nasal cavity to the PPF via the sphenopalatine foramen,
from where it can further extend to the orbit via the inferior orbital fissure or masticator space via the pterygomaxillary fissure.
Along the maxillary nerve it can further spread to the intracranial space.
The same type of spread can be seen in juvenile nasopharyngeal angiofibroma (JNA).
It is a local agressive vascular tumor which originates in the sphenopalatine fissure where it can directly invade the PPF and spread to the communicating structures.
Two muscular tumours who invade the PPF directly are fibrosarcoma and rhabdomyosarcoma who originate in the masticator space and spread through the pterygomaxillary fissure to the PPF.
The PPF then acts as a highway for further spread of disease.
Another not malignant but often life-threatening disease who uses the same pattern of spread is invasive fungal sinusitis.
It is a progressive disease that commonly occurs in immuno-comprimised patients.
The fungus can directly invade the PPF out of the paranasal sinusses and spread along the nerves to the cranial fossa where it can cause thrombosis,
infarcts,
arterial mycotic aneurysms and abscesses.
Magnetic Resonance Imaging (MRI) is the best entity to evaluate PNS because of the great contrast resolution and sensibility to discard segmental nerve affectation.
T1-weighted high resolution volumetric sequences with or without fat saturation are used.
Fat saturation allows us to define enhanced lesions that are close to spaces with fat like pterygopalatine fissure,
orbit and neurovascular foramina.
It should be mentioned that air in fat-saturation imaging may cause important susceptibility artifacts,
making diagnosis more difficult.
CT is the entity of choice to evaluate the shape and size of the foramina or canals.
RADIOLOGICAL FINDINGS OF PNS
- DIRECT SIGNS:
- Complete enhancement of the entire nerve (T1w with Gadolinium)
- Thickening or enlargement of the normal nerve caliber
- INDIRECT SIGNS:
- Obliteration of the adjacent fat pads
- Size increase of foramina and bone canals (best seen on CT)
- Muscle atrophia due to denervation
- Direct invasion by tumor
Beware of skip-lesions since PNS can seem discontinious on imaging.
This is why the nerve must be evaluated from its origin to the periphery.
C.
ANATOMY OF THE NERVES INVOLVED IN PNS
C.1.
Trigeminal nerve (V)
The trigeminal nerve originates from three sensory nuclei and one motor nucleus extending from the midbrain to the medulla.
At the level of the pons, they merge into the trigeminal ganglion (Gasser ganglion) that is located lateral to the cavernous sinus in a temporal bone depression known as Meckel's cave.
There it gives rise to three divisions: ophthalmic nerve (V1),
maxillary nerve (V2) and mandibular nerve (V3).
The ophthalmic nerve (V1) travels lateral to the cavernous sinus and exits the Meckel's cave via the superior orbital fissure.
It give rise to 3 terminal branches: frontal,
lacrimal and nasal nerves.
The maxillary nerve (V2) travels also lateral to the cavernous sinus exiting the cranium via the round foramen or foramen rotundum towards the pterygopalatine fissure.
Then it reaches to the outside and to get into the inraorbital nerve canal.
At the end of the canal it emerges into 3 terminal branches.
Two important branches along its tract are the sphenopalatine nerves and the palatine nerves.
The sphenopalatine nerves sprout from the V2 in the pterygopalatine fossa wher they contact the pterygopalatine ganglion (PPG) located in front of the Vidian nerve to which it is also connected.
The PPG has sympathic branches that innervate the bucco-pharyngeal mucosa and the lacrimal gland,
which anastomose with the lacrimal nerve branch of CN Va.
The palatine nerves also arise in the PPF and move through the greater and lesser palatine canal to the palate.
The mandibular nerve (V3) exits the Gasser's ganglion in the Meckel's cave via the foramen ovale entering the infra-temporal fossa.
Here it gives rise to the anterior trunk or buccal nerve and the posterior trunk that divides into three terminal branches: auriculotemporal nerve (ATN),
inferior alveolar nerve and lingual nerve.
The ATN passes through the parotid gland where it anastomoses with branches from the facial nerve (CN VII).
The lingual nerve runs under the tongue espace.
It connects to the chorda tympani branch of the facial nerve.
C.2 Facial nerve (VII)
The facial nerve arises in the pons.
It begins as two roots that travel through the internal meatus acousticus in the petrous part of the temporal bone.
The root leaves the internal meatus and enters the facial canal.
Within the canal,
the two roots fuse to form the facial nerve, the nerve forms the geniculate ganglion and the nerve gives rise to the greater superficial petrosal nerve (GSPN), the nerve of the stapedius and the chorda tympani.
The facial nerve then exits the canal via the stylomastoid foramen to make up the pes anserinus in the parotid gland.
The branches of the pes anserinus are responsible for innervation of the muscles of facial expression.
The greater superficial petrosal nerve (GSPN) emerges from the geniculate ganglion,
moves forward and then anastomoses with the large deep petrosal nerve (LDPN) to make up the Vidian nerve.
The chorda tympani is the anastomosis between the mastoid portion of the facial nerve,
running through the middle ear towards the Glaserian fissure to the lingual nerve 2 cm below the skull base.
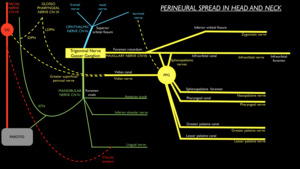
Fig. 7: Scheme of the main branches of the trigeminal nerve (yellow, blue and green).
It shows the anastomoses between the trigeminal nerve and Facial nerve and glossopharyngeal nerve to where disease can spread (perineural spread).
Important connection between the pterygopalatine ganglion (PPG) and the geniculate ganglion (GG) are the greater superficial petrosal nerve and Vidian nerve.
Another important anastomosis is the chorda tympani between the facial nerve and lingual nerve (CNV3).
An important anastomosing crossroad is the parotid gland where the facial nerve runs through and were branches of the auriculotemporal nerve (CNV3) are anastomosing.
The glossopharyngeal nerve connects with the facial nerve through the lesser deep petrosal nerve (lDPN) and with the Vidian nerve through the Large deep petrosal nerve (LDPN).
References: G-J Allemeersch, UZ Brussel - Brussel/BE
D. POSTOPERATIVE FINDINGS AT THE PPF
The pterygopataine fossa is commonly disrupted during surgery of large tumours.
After surgical violation,
the PPF almost always appears abnormal on MRI with persistent abnormal soft tissue and often enhancement within.
These expected image findings of scar tissue may be misdiagnosed as residual or reccurent disease.
Therefore it is important to obtain an early post-operative baseline scan and serial imaging for stability of findings,
absence of new lesions and absence of PNS.
E.
PATHOLOGICAL CASES INVOLVING THE PPF
E.1 Adenoid cystic carcinoma (ACC)
A 69-year-old man with a history of a nasopharyngeal adenoid cystic carcinoma for which he was treated with radiotherapy presents at follow-up.
The follow-up imaging shows invasion of the pterygopalatine fossa (PPF) ( Fig. 6 ). The PNS tracks backwards on the Vidian nerve through the Vidian canal ( Fig. 6 ) and reaches the foramen lacerum.
No pathological enhancement is seen at the level of the GSPN or facial nerve.
There is also perineural spread from the PPF to the maxillary nerve ( Fig. 8 ) running backwards through the foramen rotundum to Meckel's cave.
There is also pathologic enhancement of the infraorbital nerve due to antegrade PNS from V2 ( Fig. 8 ).
Discrete pathological enhancement is seen at the inferior half of Gasser's ganglion ( Fig. 9 ).
From there antegrade spread along V3 (mandibular nerve) is seen as a thick enhancing nerve ( Fig. 9 ). A secondary finding demonstrating involvement of the mandibular nerve is the acute denervation of the lateral pterygoid muscle ( Fig. 10 ).
This is characterized by a hyperintense appearance of the muscle and diffuse enhancement after gadolinium administration.
The fact that PNS can spread antegrade as well as retrograde is very important for the radiologist to know,
so that PNS loops can be identified and explained.
The illustrative diagram ( Fig. 11 ) shows an overview of the PNS in this case.
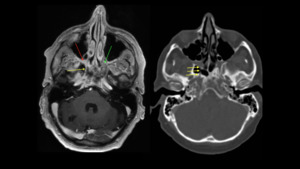
Fig. 6: Left : T1w image with gadolinium showing pathologic enhancement of the PPF, due to tumoral spread of ACC (red arrow) on the right side. Compare to a normal fat-containing PPF on the left side (green arrow). Note the lateral extension through the pteryogomaxillary fissure towards the infratemporal fossa. The yellow arrow demonstrates perineural spread along the Vidian nerve in the Vidian canal reaching the foramen lacerum.
Right: non-enhanced CT image at the same level showing the Vidian canal on a bony mesentery in the right sphenoid sinus (variant course).
References: Yannick De Brucker, Department of Radiology, UZ Brussel - Brussels/BE
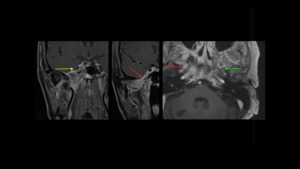
Fig. 9: LEFT : Coronal T1w fat-saturated image after gadolinium administration showing discrete partial enhancement of the inferior half of Gasser's ganglion (yellow arrow). This is due to PNS from the PPF via V2 to Meckel's cave.
MIDDLE : Coronal T1w fat-saturated image after gadolinium slightly anterior to the left image. It shows pathological enhancement and enlargement of V3 (red arrow), due to antegrade PNS from Gasser's ganglion.
RIGHT : Axial T1w fat-saturated image after gadolinium showing the PNS along the right V3 at the level of the foramen ovale. Compare to the normal mandibular nerve on the left.
References: Yannick De Brucker, Department of Radiology, UZ Brussel - Brussels/BE
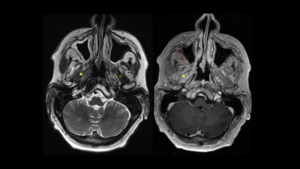
Fig. 10: Axial T2w image (left) and axial T1w image with gadolinium showing acute denervation of the right lateral pterygoid muscle. This is characterised by diffuse T2 hyperintensity and enhancement after gadolinium of the muscle (whole yellow star). The normal T2 muscle intensity is shown by the hollow yellow star. Denervation of the lateral pterygoid muscle is due to involvement of perineural spread of the ACC along the mandibular nerve.
References: Yannick De Brucker, Department of Radiology, UZ Brussel - Brussels/BE
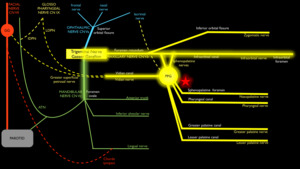
Fig. 11: Illustrative diagram of the PNS caused by the adenoid cystic carcinoma shown by the highlighted tract. Star : ACC.
References: Yannick De Brucker, Department of Radiology, UZ Brussel - Brussels/BE
E.2.
Sphenoidal meningioma with intraosseous extension and PNS
We present a case of a 62-year-old woman diagnosed with an intraosseous sphenoidal meningioma,
for which she had had a debulking surgery of a major intracranial part of the tumor.
This case illustrates the fact that PNS not only occurs in malignant tumors,
but also may be seen occasionally in benign tumors.
The tumor directly invades the cavernous sinus and the inferior half of Gasser's ganglion and causes deformation of the ganglion and pathological enhancement of this inferior part (Fig. 12).
From there the tumor spreads along the maxillary nerve through the foramen rotundum and extends into the PPF where the pterygopalatine ganglion rests ( Fig. 13 ).
The PNS then loops back along the Vidian nerve ( Fig. 14 ) through the pterygoid canal and further on to involve the entire GSPN up to the geniculate ganglion (level of the first genu of the facial nerve) ( Fig. 15 ) .
The facial nerve itself does not show pathological enhancement.
The tumor also spreads along the mandibular nerve through the foramen ovale to reach the masticator space ( Fig. 16 ).
In this space it causes lateral displacement and possible invasion of the lateral pterygoid muscle ( Fig.
16 ).
The PNS continues forward to the inferior alveolar nerve,
with obscuration of the fat pad at the mandibular foramen (not shown here).
The illustrative diagram ( Fig. 18 ) shows an overview of the PNS in this case.
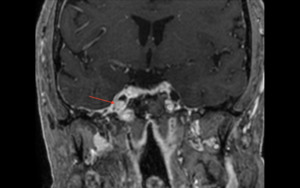
Fig. 12: Coronal T1w image with gadolinium : Direct invasion by the sphenoidal meningioma of the inferior half of Gasser's ganglion (red arrow)
References: Yannick De Brucker, Department of Radiology, UZ Brussel - Brussels/BE
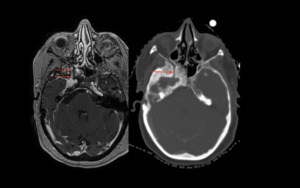
Fig. 13: Left image : Axial T1w image with gadolinium demonstrating the pathological Gasser's ganglion with perineural spread through the foramen rotundum along the maxillary nerve (red arrows) to end up in the pterygopalatine fossa.
Right image : Axial CT image of the same patient showing the secondary sclerotic bone remodelling due to the intra-osseous meningioma. The round foramen (red arrow) is widened due to the perineural spread along the maxillary nerve.
References: Yannick De Brucker, Department of Radiology, UZ Brussel - Brussels/BE
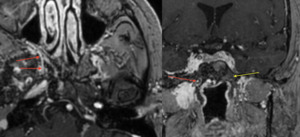
Fig. 14: Axial (left image) and coronal (right image) GT1w with gadolinium.
On these images we see pathological enhancement along the Vidian nerve (red arrow) in the pterygoid canal, indicative of PNS. The tumor tracts along the maxillary nerve, reaches the PPF and loops back via the Vidian nerve.
Yellow arrow : normal Vidian nerve/canal
References: Yannick De Brucker, Department of Radiology, UZ Brussel - Brussels/BE
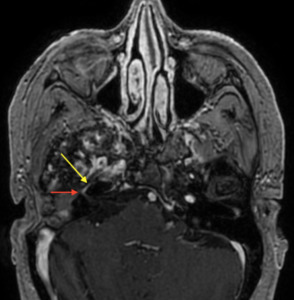
Fig. 15: Axial T1w image with gadolinium-enhanced showing perineural spread along GSPN (yellow arrow) and extending up to the geniculate ganglion of the facial nerve (red arrow).
References: Yannick De Brucker, Department of Radiology, UZ Brussel - Brussels/BE
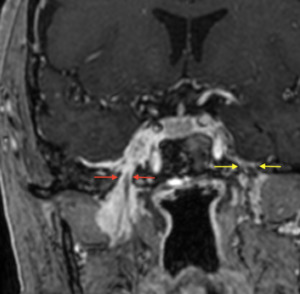
Fig. 16: Coronal T1w image with gadolinium showing the right-sided sphenoidal meningioma - which invaded the cavernous sinus and Meckel's cave with Gasser's ganglion - to track along the course of the right V3 nerve. The red arrows indicate the foramen ovale with pathological enhancement along V3. The left oval foramen is normal ( yellow arrows ).
References: Yannick De Brucker, Department of Radiology, UZ Brussel - Brussels/BE
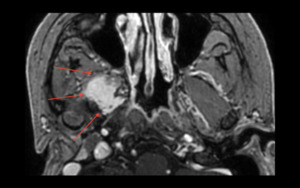
Fig. 17: Axial T1w image with gadolinium showing extension of the meningioma to the right masticator space with lateral displacement (and possible invasion) of the lateral pterygoid muscle.
References: Yannick De Brucker, Department of Radiology, UZ Brussel - Brussels/BE
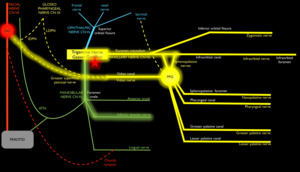
Fig. 18: Illustrative diagram of the PNS caused by the sphenoid meningioma shown by the highlighted tract. Star : meningioma with direct invasion of inferior half of Gasser's ganglion.
References: Yannick De Brucker, Department of Radiology, UZ Brussel - Brussels/BE
E.3 Squamous cell carcinoma
A 62-year-old man whith a history of a resected squamous cell carcinoma of the tip of the nose,
presents with right sided facial pain after 1 year.
At imaging a thickened and enhancing right infraorbital nerve is identified,
compatible with perineural tumor spread ( Fig. 19 ).
The PNS can be followed into the PPF ( Fig. 20 ).
From there is further retrograde perineural spread along the maxillary nerve through the foramen rotundum (Fig. 21).
No further spread to the Gasser’s ganglion was visualized neither spread was seen to the mandibular nerve or facial nerve.
The illustrative diagram ( Fig. 22 ) shows an overview of the PNS in this case.
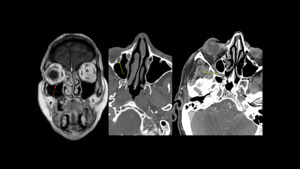
Fig. 19: LEFT : T1w coronal image with gadolinium shows a thickened and enhanced appearance of the infra-orbital nerve (red arrow) on the right side, compatible with perineural spread.
MIDDLE : Contrast-enhanced CT image in bone window shows an enlargement of the right infraorbital canal (yellow arrow), due to the perineural spread along the infra-orbital nerve. Normal infraorbital canal on the lift side.
RIGHT : Contrast-enhanced CT shows infiltration of the right pterygopalatine fossa (yellow arrow). Notice the appearance of the normal left PPF.
References: Robert Hermans MD PhD, Department of Radiology, UZ Leuven, Belgium 2016
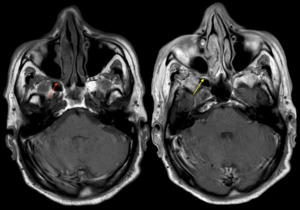
Fig. 20: LEFT : Non-enhanced T1w axial image shows a hypointense appearance of the pterygopalatine fossa (red arrows), compatible with fat replacement by retrograde PNS via the infraorbital nerve.
RIGHT : Corresponding T1w axial image with gadolinium shows enhancement of the infiltrated right PPF.
References: Robert Hermans MD PhD, Department of Radiology, UZ Leuven, Belgium 2016
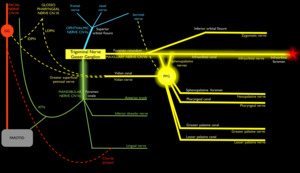
Fig. 22: Illustrative diagram of the PNS caused by the squamous cell carcinoma shown by the highlighted tract. Star : SCC at the tip of the nose
References: Yannick De Brucker, Department of Radiology, UZ Brussel - Brussels/BE
E.4 Masticator space sarcoma
A 50 year old man with a masticator space sarcoma showing extension of the sarcoma through the pterygomaxillary fissure into the PPF.
The maxillary nerve at the pterygomaxillary fissure is probably involved,
but no antegrade or retrograde PNS is seen.
There is immediate invasion of V3 by the sarcoma with retrograde PNS through the foramen ovale and extending in Meckel's cave.
Gasser's ganglion is completely involved - shown by diffuse enhancement - and further retrograde PNS is seen at the cisternal part of the trigeminal nerve up onto the pons.
Also important is the perineural spread to the auriculotemporal nerve (ATN) ( Fig. 23 ).
No pathological enhancement of the facial nerve is seen.
At clinical follow-up 3 months later,
patient is diagnosed with facial nerve paralysis,
suggesting ongoing PNS to the VIIth nerve via ATN.
The illustrative diagram ( Fig. 24 ) shows an overview of the PNS in this case.
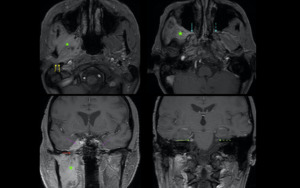
Fig. 23: UPPER LEFT : Axial T1w + Gado shows masticator space sarcoma (green star) and thick enhancing auriculotemporal nerve (yellow arrows posterior to the mandibular ramus).
UPPER RIGHT : Axial T1w + Gado shows extension of the sarcoma into the right pterygopalatine fossa (blue arrow) via the pterygomaxillary fissure (involvement of V2). Notice the normal PPF on the left (blue dotted arrow).
LOWER LEFT : Coronal T1w fat saturated + Gado shows enlarged foramen ovale with PNS along V3 (red arrow) up onto Gasser's ganglion (purple arrow). Notice the anterior section throught the normal Gasser's ganglion).
LOWER RIGHT : Coronal T1w fat saturated + Gado shows the retrograde PNS along the cisternal portion of the trigeminal right nerve (green arrow). Normal left trigeminal nerve is shown by the green dotted arrow.
References: Robert Hermans MD PhD, Department of Radiology, UZ Leuven, Belgium 2016
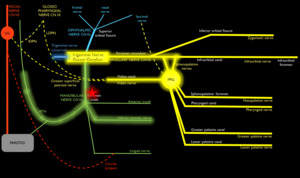
Fig. 24: Illustrative diagram of the PNS caused by the sarcoma shown by the highlighted tract. Star : masticator space sarcoma
References: Yannick De Brucker, Department of Radiology, UZ Brussel - Brussels/BE
E.5 Cystic schwannoma
A 60-year old female presents with left facial pain since several months.
On the unenhanced CT an expansile lesion is seen at the level of the left PPF.
There is scalloping of bone around,
most pronounced at the level of the middle cranial fossa.
The lesion is centered at the PPF and foramen rotundum,
indicative for a benign tumor arising from the left maxillary nerve.
The Vidian canal is also not recognised on imaging,
but lies more at the periphery of the lesion.
The foramen ovale with V3 lies immediately posterolateral to the mass.
MR imaging shows a cystic lesion with heterogenous content and fluid-fluid level,
suggestive of internal hemorrhage.
After administration of gadolinium no significant internal enhancement is seen.
No PNS was seen.
All of these findings suggest the diagnosis of cystic schwannoma of the maxillary nerve with internal hemorrhage.
The patient was operated and the diagnosis was confirmed on pathology.
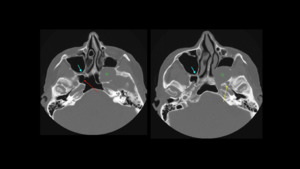
Fig. 25: Two consecutive axial NECT images at the level of the PPF (blue arrow). A large expansile lesion with benign aspect is seen at the left PPF. It scallops the bone around it. Note the close relationship of the foramen ovale (yellow arrow).
References: Robert Hermans MD PhD, Department of Radiology, UZ Leuven, Belgium 2016
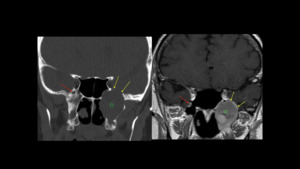
Fig. 26: LEFT : Coronal NECT image demonstrating the expansile lesion (green star) to involve the region of the left foramen rotundum. At the right side a normal foramen rotundum with maxillary nerve is seen (red arrow). The left Vidian canal is also not visible, but located more at the periphery of the lesion and probably pushed away. The scalloping nature of the lesion is shown by the yellow arrows indicating loss of bone at the middle cranial fossa below the sinus cavernosus.
RIGHT : Corresponding coronal non-enhanced T1w image at the same level.
References: Robert Hermans MD PhD, Department of Radiology, UZ Leuven, Belgium 2016
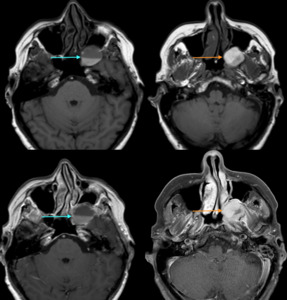
Fig. 27: The unenhanced T1w images in the upper row show a fluid-fluid level (blue arrow) and inhomogenous content of the lesion.
After administration of gadolinium (lower row) no signicant enhancement is seen (orange arrow). These findings are consistent with internal bleeding of the cystic lesion.
References: Robert Hermans MD PhD, Department of Radiology, UZ Leuven, Belgium 2016

 and lesser (yellow arrow) palatine canal with respectively the greater palatine foramen (orange curved arrow) and lesser palatine foramen (yellow curved arrow). PPF (red star). References: Gert-Jan Allemeersch, Department of Radiology, UZ Brussel - Brussels/BE")
 and lesser (yellow arrow) palatine canal from the PPF (red star) cranial to caudal (1-5). References: Gert-Jan Allemeersch, Department of Radiology, UZ Brussel - Brussels/BE")
 at the level of the Vidian canal. Communication on the lateral side with the infratemporal fossa (blue dot) via the pterygomaxillary fissure (yellow arrow) and on the medial side with the nasal cavity via the sphenopalatine foramen (green arrows).
The PPF communicates with the foramen lacerum via the Vidian canal (orange stripes).
Communication with the orbit via the infraorbital fisseure (red arrow). References: Gert-Jan Allemeersch, Department of Radiology, UZ Brussel - Brussels/BE")
. Communication of the PPF (red star) with the infratemporal fossa (blue dot) via the pterygomaxillary fissure (yellow arrow). Communication of the PPF (redstar) with the nasal cavity via the sphenopalatine forman (green arrows) on the medial side. Communication with the orbital apex via the infraorbital fissure (red arrows). References: Gert-Jan Allemeersch, Department of Radiology, UZ Brussel - Brussels/BE")
 communicating with the middle cranial fossa (yellow star) at the level of the foramen rotundum (green arrow). References: Gert-Jan Allemeersch, Department of Radiology, UZ Brussel - Brussels/BE")
 on the right side. Compare to a normal fat-containing PPF on the left side (green arrow). Note the lateral extension through the pteryogomaxillary fissure towards the infratemporal fossa. The yellow arrow demonstrates perineural spread along the Vidian nerve in the Vidian canal reaching the foramen lacerum.
Right: non-enhanced CT image at the same level showing the Vidian canal on a bony mesentery in the right sphenoid sinus (variant course). References: Yannick De Brucker, Department of Radiology, UZ Brussel - Brussels/BE")
.
It shows the anastomoses between the trigeminal nerve and Facial nerve and glossopharyngeal nerve to where disease can spread (perineural spread).
Important connection between the pterygopalatine ganglion (PPG) and the geniculate ganglion (GG) are the greater superficial petrosal nerve and Vidian nerve.
Another important anastomosis is the chorda tympani between the facial nerve and lingual nerve (CNV3).
An important anastomosing crossroad is the parotid gland where the facial nerve runs through and were branches of the auriculotemporal nerve (CNV3) are anastomosing.
The glossopharyngeal nerve connects with the facial nerve through the lesser deep petrosal nerve (lDPN) and with the Vidian nerve through the Large deep petrosal nerve (LDPN). References: G-J Allemeersch, UZ Brussel - Brussel/BE")
, due to perineural spread from the PPF (pterygopalatine ganglion) and tracking back to the Gasser's ganglion (not shown here). Green arrow points to the normal maxillary nerve on the left.
RIGHT : Axial T1w image after gadolinium administration shows the thickened enhancing right infraorbital nerve (red arrow), due to PNS of the ACC tracking forward from the maxillary nerve. References: Yannick De Brucker, Department of Radiology, UZ Brussel - Brussels/BE")
. This is due to PNS from the PPF via V2 to Meckel's cave.
MIDDLE : Coronal T1w fat-saturated image after gadolinium slightly anterior to the left image. It shows pathological enhancement and enlargement of V3 (red arrow), due to antegrade PNS from Gasser's ganglion.
RIGHT : Axial T1w fat-saturated image after gadolinium showing the PNS along the right V3 at the level of the foramen ovale. Compare to the normal mandibular nerve on the left. References: Yannick De Brucker, Department of Radiology, UZ Brussel - Brussels/BE")
 and axial T1w image with gadolinium showing acute denervation of the right lateral pterygoid muscle. This is characterised by diffuse T2 hyperintensity and enhancement after gadolinium of the muscle (whole yellow star). The normal T2 muscle intensity is shown by the hollow yellow star. Denervation of the lateral pterygoid muscle is due to involvement of perineural spread of the ACC along the mandibular nerve. References: Yannick De Brucker, Department of Radiology, UZ Brussel - Brussels/BE")

 References: Yannick De Brucker, Department of Radiology, UZ Brussel - Brussels/BE")
 to end up in the pterygopalatine fossa.
Right image : Axial CT image of the same patient showing the secondary sclerotic bone remodelling due to the intra-osseous meningioma. The round foramen (red arrow) is widened due to the perineural spread along the maxillary nerve. References: Yannick De Brucker, Department of Radiology, UZ Brussel - Brussels/BE")
 and coronal (right image) GT1w with gadolinium.
On these images we see pathological enhancement along the Vidian nerve (red arrow) in the pterygoid canal, indicative of PNS. The tumor tracts along the maxillary nerve, reaches the PPF and loops back via the Vidian nerve.
Yellow arrow : normal Vidian nerve/canal References: Yannick De Brucker, Department of Radiology, UZ Brussel - Brussels/BE")
 and extending up to the geniculate ganglion of the facial nerve (red arrow). References: Yannick De Brucker, Department of Radiology, UZ Brussel - Brussels/BE")
. References: Yannick De Brucker, Department of Radiology, UZ Brussel - Brussels/BE")
 of the lateral pterygoid muscle. References: Yannick De Brucker, Department of Radiology, UZ Brussel - Brussels/BE")

 on the right side, compatible with perineural spread.
MIDDLE : Contrast-enhanced CT image in bone window shows an enlargement of the right infraorbital canal (yellow arrow), due to the perineural spread along the infra-orbital nerve. Normal infraorbital canal on the lift side.
RIGHT : Contrast-enhanced CT shows infiltration of the right pterygopalatine fossa (yellow arrow). Notice the appearance of the normal left PPF. References: Robert Hermans MD PhD, Department of Radiology, UZ Leuven, Belgium 2016")
, compatible with fat replacement by retrograde PNS via the infraorbital nerve.
RIGHT : Corresponding T1w axial image with gadolinium shows enhancement of the infiltrated right PPF. References: Robert Hermans MD PhD, Department of Radiology, UZ Leuven, Belgium 2016")
 on the right side, compatible with retrograde PNS. Green arrow shows the contralateral normal maxillary nerve in the foramen rotundum. References: Robert Hermans MD PhD, Department of Radiology, UZ Leuven, Belgium 2016")

 and thick enhancing auriculotemporal nerve (yellow arrows posterior to the mandibular ramus).
UPPER RIGHT : Axial T1w + Gado shows extension of the sarcoma into the right pterygopalatine fossa (blue arrow) via the pterygomaxillary fissure (involvement of V2). Notice the normal PPF on the left (blue dotted arrow).
LOWER LEFT : Coronal T1w fat saturated + Gado shows enlarged foramen ovale with PNS along V3 (red arrow) up onto Gasser's ganglion (purple arrow). Notice the anterior section throught the normal Gasser's ganglion).
LOWER RIGHT : Coronal T1w fat saturated + Gado shows the retrograde PNS along the cisternal portion of the trigeminal right nerve (green arrow). Normal left trigeminal nerve is shown by the green dotted arrow. References: Robert Hermans MD PhD, Department of Radiology, UZ Leuven, Belgium 2016")

. A large expansile lesion with benign aspect is seen at the left PPF. It scallops the bone around it. Note the close relationship of the foramen ovale (yellow arrow). References: Robert Hermans MD PhD, Department of Radiology, UZ Leuven, Belgium 2016")
 to involve the region of the left foramen rotundum. At the right side a normal foramen rotundum with maxillary nerve is seen (red arrow). The left Vidian canal is also not visible, but located more at the periphery of the lesion and probably pushed away. The scalloping nature of the lesion is shown by the yellow arrows indicating loss of bone at the middle cranial fossa below the sinus cavernosus.
RIGHT : Corresponding coronal non-enhanced T1w image at the same level. References: Robert Hermans MD PhD, Department of Radiology, UZ Leuven, Belgium 2016")
 and inhomogenous content of the lesion.
After administration of gadolinium (lower row) no signicant enhancement is seen (orange arrow). These findings are consistent with internal bleeding of the cystic lesion. References: Robert Hermans MD PhD, Department of Radiology, UZ Leuven, Belgium 2016")