In order to provide a good understanding of the key imaging features in biliary obstruction we collected multiple CT and MR images from the archives of our institute.
A brief description of the epidemiology,
clinical features,
key imaging changes and differential diagnosis are provided for the most frequent benign and malignant pathologies known to generate biliary tract obstruction.
BENIGN LESIONS
I.
Choledocholithiasis
Epidemiology
• The most common benign cause of biliary tract obstruction;
• Twice more frequently encountered in women than in men (F:M = 2:1);
• The risk of developing choledocholithiasis in patients with cholelithiasis increases with age;
• Choledocholithiasis is found in up to 19 % of patients who undergo cholecystectomy [1];
• Risk factors include: pregnancy,
female gender,
family history of biliary lithiasis,
obesity,
biliary motility disorders,
rapid weight loss with extreme calorie and fat restriction or followed by a quick weight gain,
elevated serum lipid levels and use of estrogen-based oral contraceptive pills.
Clinical features
• Up to 5% of patients with choledocholithiasis are asymptomatic [2,
3];
• Primary choledocholithiasis: the stones form inside the CBD in patients who underwent cholecystectomy and in individuals with bile stasis or a recurrent infection of the bile ducts;
• Secondary choledocholithiasis: the gallstones migrate from the gallbladder and get trapped inside the CBD;
• Signs and symptoms: fluctuating obstructive jaundice,
epigastric or right hyponcondrum pain,
pruritus,
nausea,
vomiting,
dark colored urine,
pale stools [4];
• If left untreated,
it can lead to complications such as cholangitis (Charcot’s triad) or acute pancreatitis;
• Charcot’s triad: fever with rigors,
epigastric or right upper quadrant pain,
jaundice.
Key imaging changes
• Ultrasonography is used for the initial evaluation;
CT
• The sensitivity of contrast-enhanced CT for detecting choledocholithiasis is around 65-90% [5];
• Superjacent biliary tract dilatation;
• Target sign: a central rounded stone surrounded by a hypoattenuating bile;
• Crescent sign: an eccentrical crescent shape hypoattenuating bile surrounds the luminal stone;
• Possible gallstones inside the gallbladder (secondary choledocholithiasis);
• Compared to the bile,
pure cholesterol stones appear hypoattenuating while calcified stones are hyperattenuating;
• Some stones appear isoattenuating compared to the bile therefore CT cannot properly identify them;
• Examples can be seen in Fig.
1 - Fig.3.
MRI
• MRI with magnetic resonance cholangiopancreatography (MRCP) sequences tends to replace the endoscopic retrograde cholangiopancreatography (ERCP) technique for diagnosing choledocholithiasis mainly due to the similar high sensitivity (90-95%) and specificity (95-99%) rates and lack of ionising radiation or complications that often occur because of the ERCP procedure [4];
• Superjacent biliary tract dilatation;
• Possible gallstones inside the gallbladder (secondary choledocholithiasis);
• T2: well-defined stone with a low signal intensity within the CBD surrounded by a high signal intensity bile;
• MRCP: a well-defined signal void is detected within the CBD;
• Examples can be seen in Fig.
4 and Fig.
5.
Differential diagnosis
• Malignant tumors (cholangiocarcinoma,
ampullary and pancreatic head carcinoma) – suggestive clinical context (non-fluctuating painless obstructive jaundice in pancreatic head carcinoma and cholangiocarcinoma,
fluctuating obstructive jaundice in ampullary carcinoma,
unexplained weight loss without any dietary changes),
visible tumoral mass,
invaded lymph nodes,
possible secondary metastatic lesions,
possible elevated serum Carcinoembryonic Antigen,
CA 19-9,
CA 125 levels;
• Pseudotumoral chronic pancreatitis – epidemiological context (alcohol consumption,
malnutrition),
enlarged pancreas,
pancreatic calcifications or pseudocysts,
dilatation of the main pancreatic duct;
• Biliary ascariasis – epidemiological and clinical suggestive context (usually affects a large number of children,
high blood eosinophil count);
• Surgical clips;
• MRCP susceptibility artefacts.
II.
Pseudotumoral chronic pancreatitis
Epidemiology
• It is estimated that around 30% of the patients diagnosed with chronic pancreatitis develop pseudotumoral chronic pancreatitis,
out of which up to 14% are diagnosed with pancreatic adenocarcinoma during follow-up,
mainly located in the head region of the pancreas [6,
7];
• Men over 40 with long-term alcohol abuse are most frequently affected;
• Risk factors include: long-term alcohol excessive consumption (70%),
malnutrition,
gallstones obstructing the main pancreatic duct,
smoking,
hyperparathyroidism (generating elevated blood levels of calcium),
hypertriglyceridemia,
autoimmune disease and genetic factors.
Clinical features
• Signs and symptoms: abdominal pain mostly located in the epigastric region,
obstructive jaundice,
unexplained weight loss without any dietary changes,
nausea,
vomiting,
steatorrhea due to malabsorption (loss of exocrine function),
diabetes (loss of endocrine function),
dark colored urine,
pale stools.
Key imaging changes
• Ultrasonography is used for the initial evaluation;
CT and MRI
• Enlarged pancreas (mainly targeting the pancreatic head) due to a non-neoplastic lesion that might mimic a pancreatic head carcinoma;
• Dilatation of the main pancreatic duct;
• Pancreatic calcifications or pseudocysts;
• Examples can be seen in Fig.
6 - Fig.
12.
Differential diagnosis
• Malignant tumors (cholangiocarcinoma,
ampullary and pancreatic head carcinoma);
• Choledocholithiasis – epidemiological and clinical suggestive context (most common benign cause of biliary obstruction,
usually affects females,
fluctuating obstructive jaundice,
patient previously known with biliary lithiasis),
multiple stones within the biliary tract;
• Biliary ascariasis.
III.
Biliary ascariasis
Epidemiology
• It is caused by Ascaris Lumbricoides,
the largest common nematode causing human ascariasis [8];
• Tipically affects children in tropical regions;
• Biliary ascariasis may be encountered in patients aged between 4 and 70;
• Women are more frequently affected than men (F:M = 3:1);
• The parasite is transmitted through consumption of infested water,
fruits and vegetables.
Clinical features
• Signs and symptoms: epigastric and right hypocondrum pain,
nausea,
vomiting,
fluctuating obstructive jaundice,
dark colored urine,
pale stools;
• High blood eosinophil count.
Key imaging changes
CT
• Can highlight a long rounded hyperattenuating structure with a central hypoattenuating area within a dilated CBD.
MRCP
• MRCP is considered to be the best non-invasive method when it comes to detecting biliary ascariasis;
• The three line sign: the worm walls are represented by two lines with low signal intensity while the central area with increased signal intensity is associated with the worm gut;
• The dilated CBD appears as a high signal intensity area surrounding the parasite.
Differential diagnosis
• Malignant tumors (cholangiocarcinoma,
ampullary and pancreatic head carcinoma);
• Choledocholithiasis;
• Pseudotumoral chronic pancreatitis;
• MRCP susceptibility artefacts.
MALIGNANT LESIONS
I.
Pancreatic head carcinoma
Epidemiology
• Around 75% of all pancreatic cancers occur within the head of the pancreas,
while 15-20% affect the body of the pancreas and only 5-10% target the pancreatic tail;
• Tipically,
men aged between 40 and 50 are targeted by pancreatic head carcinoma;
• Risk factors include: smoking,
obesity,
diabetes,
chronic pancreatitis and genetic factors;
• Histopathology reports indicate that ductal adenocarcinomas account for up to 90% of all pancreatic cancers.
Clinical features
• Difficult to diagnose until advanced stages;
• Signs and symptoms: Courvoisier’s gallbladder (enlarged gallbladder),
unexplained weight loss without any dietary changes,
non-fluctuating obstructive jaundice,
pruritus,
dark colored urine,
pale stools,
+/- epigastric and/or right hypocondrum pain;
• Can generate possible secondary metastatic lesions (liver);
• Possible elevated serum Carcinoembryonic Antigen,
CA 19-9,
CA 125 levels.
Key imaging changes
• Ultrasonography is used for the initial evaluation;
CT
• Ductal adenocarcinomas of the pancreatic head tipically appear as ill-defined tumoral masses that enhance poorly compared to the normal pancreatic tissue;
• Most of the time,
the tumoral mass is hypodense during the arterial phase,
while during the delayed phase it can become isodense compared to the rest of the pancreas;
• Double duct sign: simultaneous dilatation of the CBD and the main pancreatic duct;
• CT can evaluate tumor extension,
affected lymph nodes and secondary metastatic lesions;
• Examples can be seen in Fig.
13 - Fig.
17.
MRI,
MRCP
• T1 pre-contrast: ill-defined tumoral mass with low signal intensity compared to the normal pancreatic tissue;
• T1 post-contrast: the tumoral mass enhances poorly compared to the rest of the pancreas;
• Double duct sign: simultaneous dilatation of the CBD and the main pancreatic duct.
Differential diagnosis
• Malignant tumors (ampullary carcinoma,
cholangiocarcinoma) – suggestive clinical context (non-fluctuating painless obstructive jaundice in pancreatic head carcinoma and cholangiocarcinoma,
fluctuating obstructive jaundice in ampullary carcinoma,
unexplained weight loss without any dietary changes),
visible tumoral mass,
invaded lymph nodes,
possible secondary metastatic lesions,
possible elevated serum Carcinoembryonic Antigen,
CA 19-9,
CA 125 levels;
• Choledocholithiasis – epidemiological and clinical suggestive context (most common benign cause of biliary obstruction,
usually affects females,
fluctuating obstructive jaundice,
patient previously known with biliary lithiasis),
multiple stones within the biliary tract;
• Pseudotumoral chronic pancreatitis – epidemiological context (alcohol consumption,
malnutrition),
enlarged pancreas,
pancreatic calcifications or pseudocysts,
dilatation of the main pancreatic duct;
• Biliary ascariasis – epidemiological and clinical suggestive context (usually affects a large number of children,
high blood eosinophil count).
II.
Ampullary carcinoma
Epidemiology
• Ampullary carcinoma represents around 20 % of all biliary tract malignancies;
• It usually affects men aged between 50 and 70;
• Possible genetic risk factors;
• Histopathology reports indicate that up to 90% of all ampullary carcinomas are adenocarcinomas.
Clinical features
• Difficult to diagnose until advanced stages;
• Signs and symptoms: fluctuating obstructive jaundice (unlike the non-fluctuating obstructive jaundice encountered in pancreatic head carcinoma and cholangiocarcinoma),
pruritus,
unexplained weight loss without any dietary changes,
dark colored urine,
pale stools,
+/- epigastric pain;
• Acute pancreatitis may be the first clinical manifestation due to the obstruction of both CBD and the main pancreatic duct;
• Can generate possible secondary metastatic lesions (liver);
• Possible elevated serum Carcinoembryonic Antigen,
CA 19-9,
CA 125 levels.
Key imaging changes
• Ultrasonography is used for the initial evaluation;
• If the lesion is in early stages,
CT and MRI can only detect abnormalities such as the dilatation of the main pancreatic duct or the biliary tract;
• If the lesion is more advanced,
CT and MRI can hardly differentiate an ampullary carcinoma from a pancreatic head tumor;
• CT can also evaluate tumor extension,
affected lymph nodes and secondary metastatic lesions;
• Double duct sign: simultaneous dilatation of the CBD and the main pancreatic duct;
• ERCP – can further investigate the ductal architecture and also provide tissue samples;
• An MR image examples can be seen in Fig.
18 and Fig.
19.
Differential diagnosis
• Malignant tumors (pancreatic head carcinoma,
cholangiocarcinoma);
• Choledocholithiasis;
• Pseudotumoral chronic pancreatitis;
• Biliary ascariasis.
III.
Cholangiocarcinoma
Epidemiology
• The highest prevalence value for this type of malignancy was recorded in Southeast Asia;
• Frequently affects men in their 6th-7th decade;
• Risk factors include: multiple hepatobiliary flukes (Clonorchis sinensis,
Opisthorchis viverrini),
primary sclerosing cholangitis,
hepatolithiasis,
choledochal cysts,
hepatitis B virus,
hepatitis C virus,
liver cirrhosis,
diabetes and human immunodeficiency virus [9,
10];
• It is not uncommon for patients to develop cholangiocarcinoma in the absence of any identifiable risk factors [11];
• Cholangiocarcinoma can be located intrahepatic,
perihilar or distal,
with the latter two previously referred to as extrahepatic forms of cholangiocarcinoma;
• It affects the perihilar area in around 50% of all cases,
with the intrahepatic (15%),
middle (17%) and distal third of the CBD (18%) being less common [12];
• Histopathology reports indicate that adenocarcinomas account for up to 95% of all cholangiocarcinomas.
Clinical features
• Difficult to diagnose until advanced stages;
• Signs and symptoms: unexplained weight loss without any dietary changes,
non-fluctuating obstructive jaundice,
pruritus,
dark colored urine,
pale stools,
+/- epigastric and/or right hypocondrum pain;
• Can generate possible secondary metastatic lesions (liver,
lungs);
• Possible elevated serum Carcinoembryonic Antigen,
CA 19-9,
CA 125 levels.
Key imaging changes
• According to the macroscopic growth pattern,
cholangiocarcinoma can be divided into the following types: mass-forming,
periductal infiltrating and intraductal [Fig.
20];
• Ultrasonography is used for the initial evaluation;
CT,
MRCP
• Mass-forming type:
- pre-contrast scans usually reveal a homogeneously hypoattenuating tumoral mass;
- post-contrast scans typically highlight a heterogeneous minor peripheral enhancement gradually progressing towards the center;
- distal dilatation of the biliary tract and capsular retraction may be present;
- the portal vein can be narrowed but,
unlike hepatocelullar carcinoma,
tumor thrombus is rarely encountered in cholangiocarcinoma.
• Periductal infiltrating type:
- the affected duct appears either narrowed or dilated;
- the hepatic periductal parenchyma usually appears thickened;
- distal dilatation of the biliary tract;
- frequently located at the hepatic hilum.
• Intraductal type:
- the duct calibre is altered;
- on pre-contrast scans a hypoattenuating tumoral mass is usually seen within the biliary tract;
- after intravenous administration of a contrast agent the mass demonstrates enhancement.
• CT can also evaluate tumor extension,
affected lymph nodes and secondary metastatic lesions.
• CT examples can be seen in Fig.
21 - Fig.
23.
• MRCP examples can be seen in Fig.
24 and Fig. 25.
Differential diagnosis
• Malignant tumors (hepatocelullar carcinoma,
ampullary and pancreatic head carcinoma);
• Multiple secondary metastatic lesions – suggestive clinical context (patient with a known advanced primary malignancy);
• Choledocholithiasis;
• Pseudotumoral chronic pancreatitis;
• Biliary ascariasis;
• Surgical clips;
• MRCP susceptibility artefacts.
IMAGE EXAMPLES
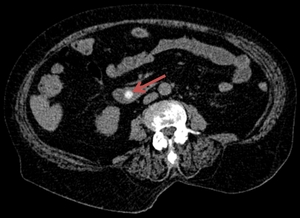
Fig. 1: The axial CT image reveals a hyperattenuating calcified stone (red arrow) within the CBD.
References: Department of Radiology Medical Imaging, University of Medicine and Pharmacy, Craiova, Romania.

Fig. 2: The coronal CT image reveals a hyperattenuating calcified stone (red arrow) within the CBD.
References: Department of Radiology Medical Imaging, University of Medicine and Pharmacy, Craiova, Romania.

Fig. 3: The axial CT image highlights a dilated CBD (blue arrow) and a mixed stone within the gallbladder (red arrow).
References: Department of Radiology Medical Imaging, University of Medicine and Pharmacy, Craiova, Romania.
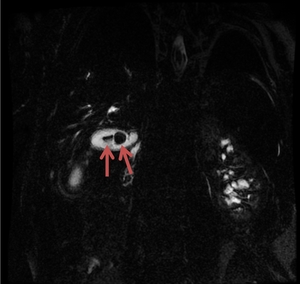
Fig. 4: The MRCP image reveals two stones within the gallbladder (red arrows).
References: Department of Radiology Medical Imaging, University of Medicine and Pharmacy, Craiova, Romania.
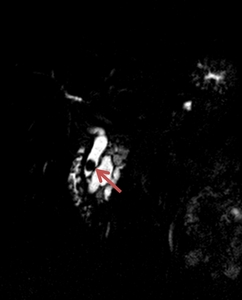
Fig. 5: The MRCP image highlights the presence of a stone within the CBD (red arrow).
References: Department of Radiology Medical Imaging, University of Medicine and Pharmacy, Craiova, Romania.

Fig. 6: The axial CT image indicates a massive calcification within an enlarged pancreatic head (red arrow).
References: Department of Radiology Medical Imaging, University of Medicine and Pharmacy, Craiova, Romania.

Fig. 7: Same patient as in Fig. 6. Axial CT image highlights the presence of calcifications within the pancreatic body and tail (red arrow).
References: Department of Radiology Medical Imaging, University of Medicine and Pharmacy, Craiova, Romania.
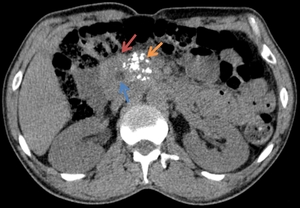
Fig. 8: The axial CT images highlight an enlarged pancreatic head (red arrow), with calcifications (yellow arrow) and a pseudocyst (blue arrow).
References: Department of Radiology Medical Imaging, University of Medicine and Pharmacy, Craiova, Romania.
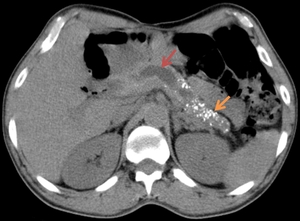
Fig. 9: Same patient as in Fig. 8. The axial CT image points towards a dilatation of the main pancreatic duct (red arrow) accompanied by pancreatic body and tail calcifications (yellow arrow).
References: Department of Radiology Medical Imaging, University of Medicine and Pharmacy, Craiova, Romania.

Fig. 10: The axial CT examination reveals a non-enhancing well-defined cystic lesion within the pancreatic head. The patient was known with chronic pancreatitis. This aspect is suggestive for a pseudocyst of the pancreatic head.
References: Department of Radiology Medical Imaging, University of Medicine and Pharmacy, Craiova, Romania.

Fig. 11: The MRI image demonstrates a round, homogeneous, high signal intensity lesion on a T2w image (red arrow) in a patient known with chronic pancreatitis. This aspect is suggestive for a pseudocyst within the pancreatic head.
References: Department of Radiology Medical Imaging, University of Medicine and Pharmacy, Craiova, Romania.
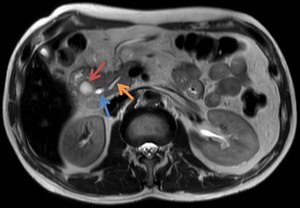
Fig. 12: Same patient as in Fig. 11. The red arrow marks the location of the pseudocyst, the blue arrow indicates the CBD and the yellow arrow indicates the main pancreatic duct.
References: Department of Radiology Medical Imaging, University of Medicine and Pharmacy, Craiova, Romania.
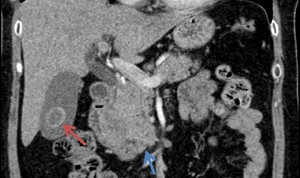
Fig. 13: The coronal CT image highlights a mixed stone (red arrow) within the gallbladder while the blue arrow points towards an ill-defined, heterogeneously enhancing pancreatic head carcinoma.
References: Department of Radiology Medical Imaging, University of Medicine and Pharmacy, Craiova, Romania.

Fig. 14: Same patient as in Fig. 13. The axial CT image highlights the ill-defined, heterogeneously enhancing pancreatic head carcinoma (red arrow).
References: Department of Radiology Medical Imaging, University of Medicine and Pharmacy, Craiova, Romania.
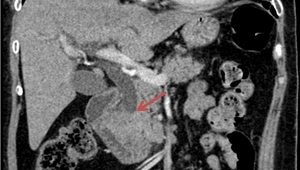
Fig. 15: The coronal CT image highlights a dilated distal CBD (red arrow) that is invaded by a pancreatic head malignant tumor.
References: Department of Radiology Medical Imaging, University of Medicine and Pharmacy, Craiova, Romania.

Fig. 16: The coronal CT image demonstrates an ill-defined hypoattenuating lesion within the pancreatic head (red arrow). The patient was diagnosed with pancreatic head carcinoma.
References: Department of Radiology Medical Imaging, University of Medicine and Pharmacy, Craiova, Romania.

Fig. 17: Same patient as in Fig. 16. The axial CT image highlights the aspect of the pancreatic head carcinoma (red arrow).
References: Department of Radiology Medical Imaging, University of Medicine and Pharmacy, Craiova, Romania.
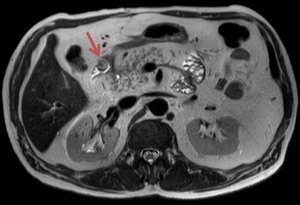
Fig. 18: The pre-contrast T2w MR image reveals a high signal intensity polypoid mass protruding into the duodenum. The patient was diagnosed with ampullary carcinoma.
References: Department of Radiology Medical Imaging, University of Medicine and Pharmacy, Craiova, Romania.
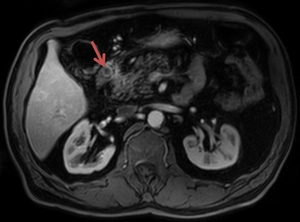
Fig. 19: Same patient as in Fig. 18. After intravenous administration of a contrast agent, the polypoid mass demonstrates a moderate enhancement (mostly peripheral) during the arterial phase (~20 sec).
References: Department of Radiology Medical Imaging, University of Medicine and Pharmacy, Craiova, Romania.
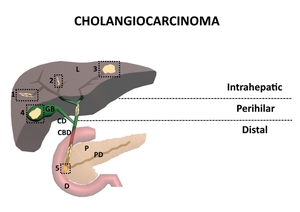
Fig. 20: Types of cholangiocarcinoma. 1. Periductal infiltrative; 2. Intraductal; 3. Mass-forming; 4. Carcinoma of the gallbladder; 5. Ampullary carcinoma; L – Liver; GB – Gallbladder; CD – Cystic duct; CBD – Common bile duct; P – Pancreas; PD – Pancreatic duct; D - Duodenum
References: Florescu LM, Florescu DN, Gheonea IA. The Importance of Imaging Techniques in the Assessment of Biliary Tract Cancer. J Med Life. 2017 July-Sep. pp. 201-208
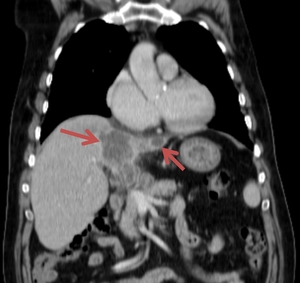
Fig. 21: The abdominal CT examination of a 59 year old male pacient revealed a hypoattenuating area showing low contrast enhancement, mostly peripheral, located in the right hepatic lobe, suggesting an intrahepatic form of cholangiocarcinoma. A similar lesion was described in the left hepatic lobe.
References: Florescu LM, Florescu DN, Gheonea IA. The Importance of Imaging Techniques in the Assessment of Biliary Tract Cancer. J Med Life. 2017 July-Sep. pp. 201-208
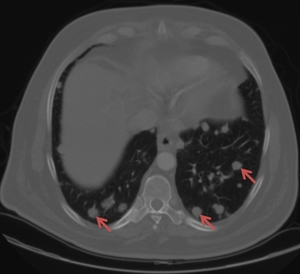
Fig. 22: Same patient as in Fig. 21. The red arrows are indicating multiple pulmonary metastases.
References: Florescu LM, Florescu DN, Gheonea IA. The Importance of Imaging Techniques in the Assessment of Biliary Tract Cancer. J Med Life. 2017 July-Sep. pp. 201-208

Fig. 23: The abdominal CT examination of a 79 year old female pacient revealed a hypoattenuating area showing low contrast enhancement located in the right hepatic lobe, just above the gallbladder, suggesting a perihilar cholangiocarcinoma.
References: Florescu LM, Florescu DN, Gheonea IA. The Importance of Imaging Techniques in the Assessment of Biliary Tract Cancer. J Med Life. 2017 July-Sep. pp. 201-208

Fig. 24: An MRCP examination performed on a 72 year old male pacient revealed choledochal lithiasis accompanied by an extrahepatic cholangiocarcinoma (red arrow) that extended towards the common bile duct, just before the emergence of the cystic duct.
References: Florescu LM, Florescu DN, Gheonea IA. The Importance of Imaging Techniques in the Assessment of Biliary Tract Cancer. J Med Life. 2017 July-Sep. pp. 201-208
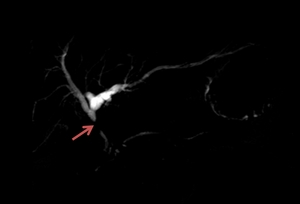
Fig. 25: An MRCP examination performed on a 69 year old male pacient revealed complete obstruction of the common bile duct on 12 mm length, accompanied by superjacent dilatation of the biliary tract, suggesting an extrahepatic form of cholangiocarcinoma.
References: Florescu LM, Florescu DN, Gheonea IA. The Importance of Imaging Techniques in the Assessment of Biliary Tract Cancer. J Med Life. 2017 July-Sep. pp. 201-208
