Anatomy and Embryology
The pancreas and biliary tract are anatomically and embryologically related to each other.
These organs are anatomically adjacent to each other and,
embryologically,
both arise from the foregut endoderm almost at the same time.
The ventral pancreas develops from the biliary primordium and fuses with the dorsal pancreas to form the pancreas.
Moreover,
the pancreas and biliary tract share the same transcription factors during their development process.
Among these transcription factors,
reduced HES1 expression is considered to inhibit the development of the pancreas and result in an abnormal biliary tract,
possibly leading to disease formation.
Accessory glands are distributed along the pancreatic duct and biliary tract.
Some of the accessory glands around the biliary tract are exocrine pancreatic glands.
Based on these findings,
the biliary tract can be regarded as an incomplete pancreatic tissue.
In fact,
some biliary diseases have similar characteristics to pancreatic diseases and are referred to as "biliary diseases with pancreatic counterparts".
To illustrate intraductal papillary neoplasms of the pancreas,
bile duct,
gallbladder,
and ampulla by contrasting the CT/MRI images with histological findings.
IPMN(intraductal papillary mucinous neoplasm)
Pathology
IPMN are mucin-producing tumors arising from the epithelium of the pancreatic duct (main duct type),
its side branches (side branch type),
or mixed (combined type) .
Subtypes
- Main duct IPMN
- Side branch IPMN
- Mixed IPMN
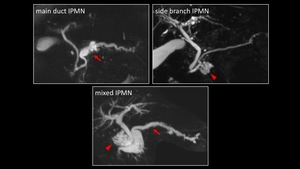
Fig. 2: Subtypes of IPMN
Clinical features
2-20% of patients can be symptomatic.
(abdominal pain,
pancreatitis and diabetes mellitus.)
Epidemiology
IPMN typically presents in men (70%) and in the older age group,
with a mean age of 65 years.
Increasing incidentally detected and surgically resected.
Imaging
- Main duct IPMN:segmental or diffuse dilation of main pancreatic duct (>5mm),without a visible obstructing lesion or stenosis.
- Side branch IPMN:cysts measuring >5mm in diameter which communicate with the main pancreatic duct; often seen as grape like cluster of cysts.
Most common location is head and neck; often multifocal.
- Mixed IPMN:combines both types.
Accuracy of MDCT in characterization :24-61%.
Accuracy of MRI is 74%
Prognosis
Risk of malignancy (Main duct IPMN: 38〜68%.
Side branch IPMN: 12〜47%.
Mixed IPMN: 38〜65%)
5 year survival for noninvasive IPMN: 90-100%
5 year survival for invasive IPMN: 31-60%
IPMN arises through an adenoma-carcinoma sequence,
where the malignancy grade increases in a stepwise manner.
IPMN has a wide spectrum of variants resulting from mutations of the GNAS and KRAS genes.
The current guidelines recommend assessing the malignancy grade of IPMN based on high-risk stigmata and worrisome features.
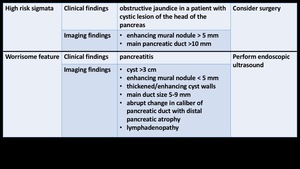
Fig. 3
Although IPMN is a risk factor for pancreatic cancer development,
pancreatic carcinomas can arise from not only IPMNs (IPMN-derived pancreatic carcinoma),
but also from non-IPMN areas (IPMN-concomitant pancreatic carcinoma).
The prevalence of IPMN-concomitant pancreatic carcinoma has been reported as 1.9-9.2%.
Advanced age,
female sex,
undilated main pancreatic duct,
and small size of cysts are associated with an increased incidence.
The detection of new-onset or worsening diabetes or increased CA19-9 levels during the follow-up can also lead to the diagnosis.
On imaging,
stenosis of the main pancreatic duct on MRCP and a high-intensity signal on DWI can lead to the detection of this lesion.
Especially,
follow-up with imaging studies is important,
as concomitant carcinomas can arise metachronously even after IPMN removal.
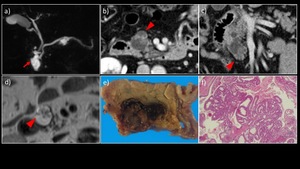
Fig. 4: A 60-year-old man with branch type IPMN (pancreatic head) and gastric type IPMN with mild to moderate atypia with no invasion
a) MRCP MIP image showed a multilocular cystic lesion communicating with the main pancreatic duct in the pancreatic head (→) and the pancreatic body. There was no dilatation of the main pancreatic duct. b) Contrast-enhanced CT. c) Coronary section showed an enhanced solid component measuring 30 mm in maximum diameter within the cyst in the pancreatic head (▶). d) T2WI showed an elevated papillary lesion in the cyst in the pancreatic head (▶). e) The extracted specimen showed that the cystic lesion with a mural nodule was in communication with the dilated accessory pancreatic duct. f) HE staining with high power magnification showed proliferation of mild to moderate atypical glands in the mural nodule.
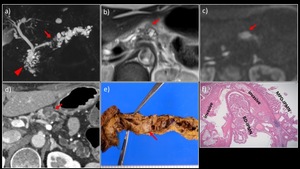
Fig. 5: A 70-year-old woman with mixed-type IPMN-derived pancreatic carcinoma in the pancreatic body.
a) MRCP MIP showed an interruption of the main pancreatic duct in the pancreatic body (→), as well as a dilated upstream pancreatic duct and multiple cysts. A multilocular cystic lesion was also detected in the pancreatic head (▶). b) MRI T2WI revealed a multilocular cystic lesion with mural nodules in the pancreatic body (→). c) On DWI (b = 1000 s/mm2), attenuated diffusion was observed. d) Contrast-enhanced CT showed delayed enhancement of the nodule. e) The resected specimen contained a white-colored solid component in the pancreatic body (→). f) HE-stained magnified image showed findings of mixed-type IPMN and interstitial invasion by atypical glandular ducts.
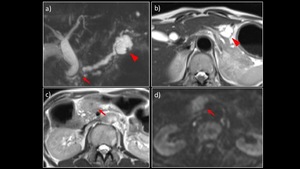
Fig. 6: A 60-year-old woman with IPMN-concomitant pancreatic carcinoma.
a) MRCP MIP showed an interruption of the main pancreatic duct in the pancreatic body (→) and a dilated upstream pancreatic duct. A 30-mm branched IPMN was detected in the pancreatic tail (▶). b), c) MRI T2WI revealed a branched IPMN in the pancreatic body (▶) and a solid mass in the pancreatic head (→). d) On DWI (b = 1000 s/mm2), the lesion in the pancreatic head showed attenuated diffusion. The lesion in the pancreatic head was biopsied under EUS guidance and confirmed to be an adenocarcinoma.
IPNB(intraductal papillary neoplasm of bile duct)
Pathology
IPNB is a disease group consisting of tumors that undergo papillary proliferation into the bile duct lumen (including tumors formerly referred to as bile duct papillomatosis,
mucus-producing bile duct tumor,
papillary adenocarcinoma of the extrahepatic bile duct,
and non-invasive intraductal growth-type intrahepatic cholangiocarcinoma).
IPNB occurs in the extrahepatic bile ducts and large intrahepatic bile ducts,
infrequently at multiple sites.
IPNB may or may not produce mucus; mucus overproduction is observed in approximately 30% of cases.
IPNB is regarded as a precancerous or preinvasive cancerous lesion of the biliary system.
The degree of dysplasia can be mild (adenoma grade) to severe (carcinoma in situ grade),
reflecting the stepwise carcinogenic process of bile duct carcinomas (attributed to GNAS1 gene mutations).
Subtypes
- Ductal dilatation-type:
- Mucus overproduction-type (cyst-type):
- Non-mucus overproduction-type
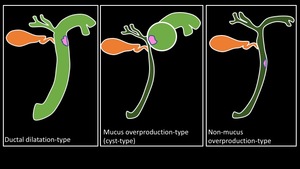
Fig. 7: Subtypes of IPNB
Clinical features
Right upper quadrant pain,
recurrent cholangitis,
jaundice,
and anemia.
Increased CA19-9 and CEA levels were observed.
Epidemiology
IPNB common seen in adult men (M:F 2:1) with a mean age of 60-65years.
Imaging
- Ductal dilatation-type: A mass protruding into the bile duct lumen that causes mucobilia through mucus production. Dilatation of bile ducts up- and downstream of the mass.
- Mucus overproduction-type (cyst-type): A mono- or multi-locular mass with papillary growth in the cystic lumen. May or may not have communication with the bile ducts.
- Non-mucus overproduction-type: An intraductal papillary mass without ductal dilatation.
Prognosis
IPNB are associated with a better prognosis compared with that for nonpapillary cholangiocarcinomas.
5 year survival for IPNB: 47%
The prognosis of IPNB with mucin secretion is better than that of IPNB without mucin secretion.
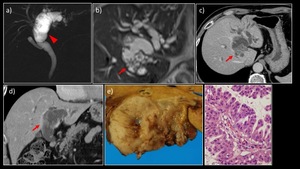
Fig. 8: A 70-year-old man with intrahepatic IPNB (bile duct dilatation type)
a) MRCP MIP image showed significant dilatation in the region from the left hepatic duct to the common bile duct (▶). b) MRI T2WI showed a papillary lesion protruding into the dilated duct with mucobilia (→). c) Contrast-enhanced CT. d) Coronary section also showed a papillary lesion protruding into the bile duct (→). The contrast enhancement was less marked than that of the hepatic parenchyma. e) The extracted specimen showed a tumor filling the dilated bile duct, mainly in the area of the left hepatic duct. f) Histological examination showed papillary proliferation of atypical glands containing eosinophilic granular cells along with overproduction of mucus.
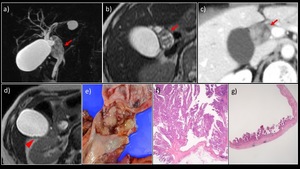
Fig. 9: A 70-year-old woman with IPNB + ICPN
a) MRCP MIP image. b) MRI T2WI revealed a 4 × 2-cm nodule showing papillary growth in the dilated cystic duct (→), partially protruding into the middle bile duct. No dilatation of the bile ducts, including the lower bile duct, was observed. c) Contrast-enhanced dynamic CT revealed a nodule in the focally dilated cystic duct that was gradually, weakly, and evenly enhanced. d) A tiny nodule showing papillary growth was also detected in the gallbladder (▶). e) The resected specimen contained a papillary mass (an IPNB-like mass) occupying the cystic duct lumen. f) The histological diagnosis was papillary adenocarcinoma (pap) (= IPNB, non-invasive carcinoma, oncocytic type), with an invasion depth of pTis. g) The lesion in the gallbladder was histologically diagnosed as papillary adenocarcinoma (pap), with a local invasion depth of pTis.
ICPN(intracholecystic papillary tubular neoplasm)
Pathology
ICPN is a papillary tumorous lesion that can be macroscopically identified in the gallbladder.
ICPN is regarded as a precancerous or preinvasive cancerous lesion (premalignant lesion) of the biliary system.
This lesion can be pedunculated or subpedunculated (papillary,
nodular),
and may occur at multiple sites.
It has a fine fibrous vascular core,
with the glandular epithelium showing papillary or tubular growth.
ICPN is characterized by the proliferation of atypical glandular ducts of adenoma or low-grade adenocarcinoma grade,
which generally retains orderly arrangement,
and arises through the adenoma-carcinoma sequence.
ICPN can be classified into various cellular phenotypes,
including the pancreatobiliary,
gastric,
intestinal,
and eosinophilic cell types.
Mucus production is rarely observed,
and no necrosis is noted.
Adsay et al.
have reported the pathological features that define ICPN.
【Definition of ICPN】
- Intramucosal
- Preinvasive neoplastic (dysplasia)
- Mass forming; exophytic (papillary or polypoid)
- ≧1.0cm
- Compact
- Distinct from the neighboring mucosa
Clinical features
Often asymptomatic,
incidentally detected during cholecystectomy.
Seen in 0.5% cholelithiasis or chronic cholecystitis specimens.
An estimated 6% of GB adenocarcinomas arises in association with ICPN.
Epidemiology
ICPN common seen in adult women (F>M) with a mean age of 60 years.
Imaging
So far,
there has been no conclusive report on the imaging findings of ICPN of the gallbladder.
In all three cases of ICPN of the gallbladder encountered in our hospital,
imaging studies revealed a 2-4-cm papillary elevated lesion in the gallbladder,
with no thickening or deformity of the gallbladder wall.
Other findings included an enlarged gallbladder due to mucus production,
a single-layered high-intensity area over the tumor surface on MRI T2WI,
and strong enhancement at the base of the tumor.
In cases of gallbladder carcinoma,
abnormalities of the gallbladder wall and invasion into surrounding organs can be observed.
Gallbladder enlargement is also uncommon in cases of gallbladder carcinoma.
Thus,
the reported imaging findings may be helpful for differentiating ICPN from gallbladder carcinoma.
Prognosis
The 5-year survival rate for ICPN was significantly higher than that for conventional gallbladder carcinoma (30%).
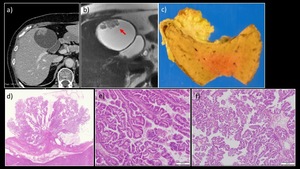
Fig. 10: A 70-year-old woman with ICPN of the gallbladder
a) Contrast-enhanced CT showed an enlarged gallbladder and an elevated papillary lesion in the fundus. There was neither wall thickening nor deformity. b) MRI T2WI (coronary section) showed a high intensity signal in the surface layer of the tumor (→). There was no dilatation of either the intrahepatic duct or the common bile duct (not shown). c) The extracted specimen showed a papillary mass lesion measuring 22 mm in maximum diameter at the fundus of the gallbladder. d)When examined with a magnifying glass, the specimen was found to contain proliferating dysplastic atypical glands with a fibrovascular core, comprising both papillary and glandular components. HE staining with high power magnification showed both e) low grade dysplasia and f) high grade dysplasia, and there were no components indicative of invasive cancer.
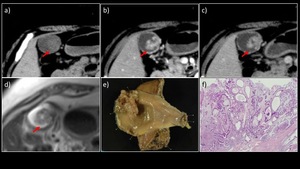
Fig. 11: A 60-year-old woman with ICPN
a) Plain, b) early-phase, and c) delayed-phage contrast-enhanced dynamic CT scans revealed a papillary elevated lesion at the base of the gallbladder, showing an early enhancement pattern. No thickening or deformity of the gallbladder wall was observed. d) On MRI T2WI, the mass exhibited a high-intensity signal. No gallbladder enlargement was observed. e) The resected specimen contained a 4-cm papillary tumorous lesion in the mucosa of the base of the gallbladder (→). f) HE-stained magnified image showed papillary or tubular proliferation of atypical glandular ducts of the intestinal phenotype, with a cellular atypism of low- to high-grade dysplasia. No invasive carcinoma component was detected.
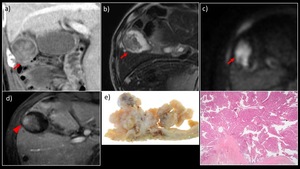
Fig. 12: A 80-year-old man with ICPN
a) Contrast-enhanced CT and b) MRI T2WI revealed a papillary elevated lesion in the gallbladder (→). c) On DWI (b = 1000 s/mm2), attenuated diffusion was observed. d) Contrast-enhanced MRI showed an intense enhancement at the base of the tumor (▶). No thickening or deformity of the gallbladder wall was observed. e) The resected specimen contained a 3-cm papillary tumorous lesion in the mucosa of the base of the gallbladder (→). f) HE-stained image showed papillary or tubular proliferation of the gastric or biliary phenotype, and partially of the oncocyte phenotype, with a cellular atypism of low- to high-grade dysplasia. No invasive carcinoma component was detected.
IAPN(intraampullary papillary tubular neoplasm)
Pathology
A localized,
papillary/polypoid,
exophilic,
elevated lesion was detected in the ampullary duct (ranging from the common duct to the ampullary bile duct/pancreatic duct),
and proliferation of glandular ducts of various malignancy grades (from adenoma to adenocarcinoma) was observed.
Mucus overproduction was rarely seen.
Adsay et al.
proposed new macroscopic classification criteria for invasive ampullary carcinomas based on the tumor localization,
morphology,
mode of carcinogenesis,
and cellular phenotype,
where intra-ampullary-type carcinomas are classified as close to IPMN/ITPN of the pancreas and IPNB of the bile duct.
Clinical features
Jaundice,
weight loss and abdominal pain
Epidemiology
IAPN common seen in adult men (M:F 2:1) with a mean age of 60 years.
25% of primarily ampulally neoplasms.
Imaging
I So far,
there has been no conclusive report on the imaging findings of IAPN.
In the cases of IAPN encountered in our hospital,
imaging studies revealed an exophilic elevated lesion in the ampullary duct,
with dilated upstream bile ducts.
No apparent extramural invasion was observed.
Prognosis
Most IAPN lesions are well-differentiated tubular adenocarcinomas,
with a low invasion depth and low rate of lymph node metastasis.
Accordingly,
IAPN is associated with a relatively good prognosis.
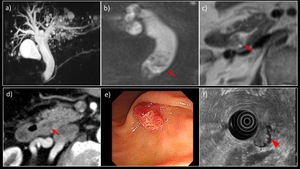
Fig. 13: A 70-year-old man with IAPN of the papilla, papillotubular adenoma
a) MRCP MIP image showed diffuse dilatation of the bile duct. There was no dilatation of the main pancreatic duct. b) MRI with fat suppression T2WI (coronary section) showed a papillary mass protruding into the distal bile duct (→). c) MRI T2WI and d) contrast-enhanced CT showed an elevated lesion in the papillary bile duct (→), with a slight but gradually increasing homogenous enhancement. e) Upper gastrointestinal endoscopy showed an erythematous elevated lesion. f) EUS showed a papillary low echoic mass measuring 15 mm in maximum diameter (▶). Biopsy was performed later and papillotubular adenoma was histologically diagnosed.
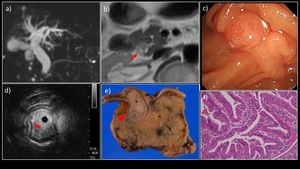
Fig. 14: A 80-year-old man with IAPN adenocarcinoma (Intraductal papillary, non-invasive)
a) MRCP MIP showed diffuse bile duct dilatation, with no dilatation of the main pancreatic duct. b) MRI T2WI revealed an elevated lesion in the distal bile duct (→). No apparent diffusion attenuation was observed. c) Upper endoscopy revealed a nodular papilla. d) EUS revealed a 15-mm low echoic mass in the ampullary bile duct (→). e) The resected specimen contained a tumorous lesion occupying the ampullary bile duct through the lower bile duct (▶); f) HE-stained magnified image showed a papillary proliferative lesion comprising atypical glandular ducts. No interstitial invasion was observed (Tis grade).



 and gastric type IPMN with mild to moderate atypia with no invasion
a) MRCP MIP image showed a multilocular cystic lesion communicating with the main pancreatic duct in the pancreatic head (→) and the pancreatic body. There was no dilatation of the main pancreatic duct. b) Contrast-enhanced CT. c) Coronary section showed an enhanced solid component measuring 30 mm in maximum diameter within the cyst in the pancreatic head (▶). d) T2WI showed an elevated papillary lesion in the cyst in the pancreatic head (▶). e) The extracted specimen showed that the cystic lesion with a mural nodule was in communication with the dilated accessory pancreatic duct. f) HE staining with high power magnification showed proliferation of mild to moderate atypical glands in the mural nodule.")
 MRCP MIP showed an interruption of the main pancreatic duct in the pancreatic body (→), as well as a dilated upstream pancreatic duct and multiple cysts. A multilocular cystic lesion was also detected in the pancreatic head (▶). b) MRI T2WI revealed a multilocular cystic lesion with mural nodules in the pancreatic body (→). c) On DWI (b = 1000 s/mm2), attenuated diffusion was observed. d) Contrast-enhanced CT showed delayed enhancement of the nodule. e) The resected specimen contained a white-colored solid component in the pancreatic body (→). f) HE-stained magnified image showed findings of mixed-type IPMN and interstitial invasion by atypical glandular ducts.")
 MRCP MIP showed an interruption of the main pancreatic duct in the pancreatic body (→) and a dilated upstream pancreatic duct. A 30-mm branched IPMN was detected in the pancreatic tail (▶). b), c) MRI T2WI revealed a branched IPMN in the pancreatic body (▶) and a solid mass in the pancreatic head (→). d) On DWI (b = 1000 s/mm2), the lesion in the pancreatic head showed attenuated diffusion. The lesion in the pancreatic head was biopsied under EUS guidance and confirmed to be an adenocarcinoma.")


a) MRCP MIP image showed significant dilatation in the region from the left hepatic duct to the common bile duct (▶). b) MRI T2WI showed a papillary lesion protruding into the dilated duct with mucobilia (→). c) Contrast-enhanced CT. d) Coronary section also showed a papillary lesion protruding into the bile duct (→). The contrast enhancement was less marked than that of the hepatic parenchyma. e) The extracted specimen showed a tumor filling the dilated bile duct, mainly in the area of the left hepatic duct. f) Histological examination showed papillary proliferation of atypical glands containing eosinophilic granular cells along with overproduction of mucus.")
 MRCP MIP image. b) MRI T2WI revealed a 4 × 2-cm nodule showing papillary growth in the dilated cystic duct (→), partially protruding into the middle bile duct. No dilatation of the bile ducts, including the lower bile duct, was observed. c) Contrast-enhanced dynamic CT revealed a nodule in the focally dilated cystic duct that was gradually, weakly, and evenly enhanced. d) A tiny nodule showing papillary growth was also detected in the gallbladder (▶). e) The resected specimen contained a papillary mass (an IPNB-like mass) occupying the cystic duct lumen. f) The histological diagnosis was papillary adenocarcinoma (pap) (= IPNB, non-invasive carcinoma, oncocytic type), with an invasion depth of pTis. g) The lesion in the gallbladder was histologically diagnosed as papillary adenocarcinoma (pap), with a local invasion depth of pTis.")
 Contrast-enhanced CT showed an enlarged gallbladder and an elevated papillary lesion in the fundus. There was neither wall thickening nor deformity. b) MRI T2WI (coronary section) showed a high intensity signal in the surface layer of the tumor (→). There was no dilatation of either the intrahepatic duct or the common bile duct (not shown). c) The extracted specimen showed a papillary mass lesion measuring 22 mm in maximum diameter at the fundus of the gallbladder. d)When examined with a magnifying glass, the specimen was found to contain proliferating dysplastic atypical glands with a fibrovascular core, comprising both papillary and glandular components. HE staining with high power magnification showed both e) low grade dysplasia and f) high grade dysplasia, and there were no components indicative of invasive cancer.")
 Plain, b) early-phase, and c) delayed-phage contrast-enhanced dynamic CT scans revealed a papillary elevated lesion at the base of the gallbladder, showing an early enhancement pattern. No thickening or deformity of the gallbladder wall was observed. d) On MRI T2WI, the mass exhibited a high-intensity signal. No gallbladder enlargement was observed. e) The resected specimen contained a 4-cm papillary tumorous lesion in the mucosa of the base of the gallbladder (→). f) HE-stained magnified image showed papillary or tubular proliferation of atypical glandular ducts of the intestinal phenotype, with a cellular atypism of low- to high-grade dysplasia. No invasive carcinoma component was detected.")
 Contrast-enhanced CT and b) MRI T2WI revealed a papillary elevated lesion in the gallbladder (→). c) On DWI (b = 1000 s/mm2), attenuated diffusion was observed. d) Contrast-enhanced MRI showed an intense enhancement at the base of the tumor (▶). No thickening or deformity of the gallbladder wall was observed. e) The resected specimen contained a 3-cm papillary tumorous lesion in the mucosa of the base of the gallbladder (→). f) HE-stained image showed papillary or tubular proliferation of the gastric or biliary phenotype, and partially of the oncocyte phenotype, with a cellular atypism of low- to high-grade dysplasia. No invasive carcinoma component was detected.")
 MRCP MIP image showed diffuse dilatation of the bile duct. There was no dilatation of the main pancreatic duct. b) MRI with fat suppression T2WI (coronary section) showed a papillary mass protruding into the distal bile duct (→). c) MRI T2WI and d) contrast-enhanced CT showed an elevated lesion in the papillary bile duct (→), with a slight but gradually increasing homogenous enhancement. e) Upper gastrointestinal endoscopy showed an erythematous elevated lesion. f) EUS showed a papillary low echoic mass measuring 15 mm in maximum diameter (▶). Biopsy was performed later and papillotubular adenoma was histologically diagnosed.")

a) MRCP MIP showed diffuse bile duct dilatation, with no dilatation of the main pancreatic duct. b) MRI T2WI revealed an elevated lesion in the distal bile duct (→). No apparent diffusion attenuation was observed. c) Upper endoscopy revealed a nodular papilla. d) EUS revealed a 15-mm low echoic mass in the ampullary bile duct (→). e) The resected specimen contained a tumorous lesion occupying the ampullary bile duct through the lower bile duct (▶); f) HE-stained magnified image showed a papillary proliferative lesion comprising atypical glandular ducts. No interstitial invasion was observed (Tis grade).")