We retrospectively reviewed cases of paediatric patients investigated for VUR at our institution from January 2013 to December 2017.
122 patients (64 males and 58 females) underwent ce-VUS with intravesical administration of SonoVue® for the indication of "antenatal diagnosed urinary pathology and/or UTIs".
Their age ranged from 4 days to 26 years (mean age: 3 years and 7 months).
We found 64 patients with VUR,
73 patients had urinary pathology and 43 presented VUR associated with urinary pathology (26 males,
17 females).
For those who presented VUR associated with urinary pathology we evaluated the imaging findings,
we graded VUR according to Darge (Table 1) and we classified them in: reno-urinary abnormalities,
anomalies of the distal ureter,
anomalies of the bladder and anomalies of the urethra.
Reno-urinary abnormalities:
Case 1: One month old boy with bilateral renal hypoplasia [right kidney (RK)=23mm,
left kidney (LK)=24mm] and dysplasia with increased parenchymal echogenicity and reduced corticomedullary differentiation.
We observed bilateral VUR grade IV.
Fig. 1
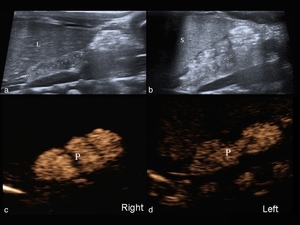
Fig. 1: Bilateral renal dysplasia and hypoplasia (L-liver;S-spleen). ce-VUS shows bilateral VUR (microbubbles in the renal pelvis - P).
References: Department of Radiology, Children Emergency Hospital, Cluj Napoca/RO.
Case 2: Five years old girl with right renal hypoplasia (RK=64mm,
LK=93mm),
bilateral renal pelvic dilatation and with an associated VUR (grade IV-right side,
grade II- left side).
Fig. 2
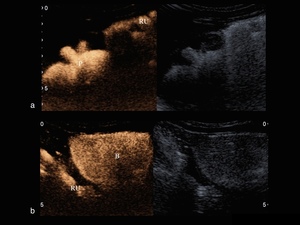
Fig. 2: Right renal hypoplasia.
ce-VUS a) Longitudinal scan of the right kidney shows the presence of microbubbles in the right renal pelvis (P) and also in the right ureter (RU);
b) Longitudinal scan of the bladder (B) shows reflux of contrast material in the RU.
References: Department of Radiology, Children Emergency Hospital, Cluj Napoca/RO.
Case 3: One month old boy with right renal dysplasia and hypoplasia (RK=38mm,
LK=45mm).
He presented uroepithelial thickening (UET) of the renal pelvis and associated right VUR (grade IV).
Fig. 3
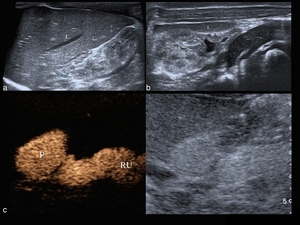
Fig. 3: Right renal dysplasia and hypoplasia.
a) Longitudinal scan - shows increased parenchymal echogenicity of the right kidney (RK) compared to the liver (L);
b) Transverse scan of the right kidney shows uroepithelial thickening (measured⇒2mm);
c) ce-VUS image shows right VUR (grade IV).
References: Department of Radiology, Children Emergency Hospital, Cluj Napoca/RO.
Case 4: Seven years old boy with "horseshoe kidney" and an associated intermittent left VUR (grade II).
Fig. 4
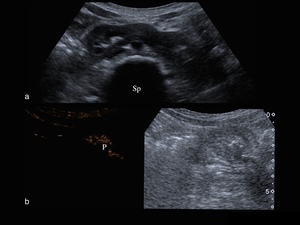
Fig. 4: Horseshoe kidney.
a) Transverse scan of the kidneys shows that the lower poles are attached in front of the aorta and the spine (Sp);
b) ce-VUS shows left VUR (grade II).
References: Department of Radiology, Children Emergency Hospital, Cluj-Napoca/RO.
Case 5: Three months old boy with right retrovesical multicystic kidney,
left pelvicalyceal dilatation and an associated left VUR (grade III). Fig. 5 ,
Fig. 6
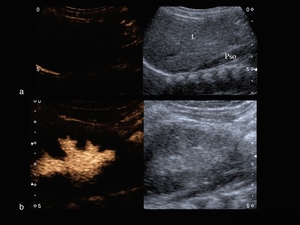
Fig. 5: Ectopic multicystic kidney. a) Longitudinal scan of the right flank - shows the absence of the right kidney in the right renal fossa, between the liver (L) and the right psoas muscle (Pso); b) Longitudinal scan of the left kidney shows the presence of microbubbles in the renal pelvis.
References: Department of Radiology, Children Emergency Hospital, Cluj-Napoca/RO.
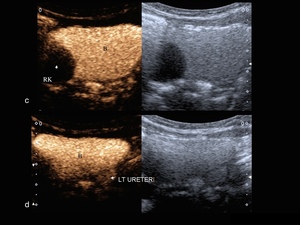
Fig. 6: c) Transverse scan of the urinary bladder (B) shows the right multicystic kidney (cyst = arrow) located posterior to it;
d) Transverse scan of the B shows reflux of contrast material in the left ureter.
References: Department of Radiology, Children Emergency Hospital, Cluj-Napoca/RO.
Case 6: Seven years old boy presented with: right renal malrotation,
left renal ectopia with an associated malrotation and bilateral VUR (grade V).
The kidneys had an increased parenchymal echogenicity,
no corticomedullary differentiation and important bilateral pelvicalyceal and ureteral dilatation.
It was also noticed an abnormally enlarged bladder.
Fig. 7
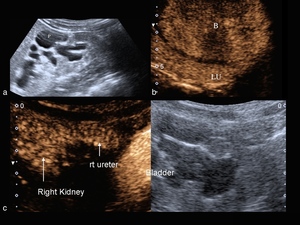
Fig. 7: Renal malrotation. a) Longitudinal scan of the right malrotated kidney - the renal pelvis (P) is located anteriorly;
b) ce-VUS shows a dilated left ureter (LU) with VUR;
c) ce-VUS shows right pelvicalyceal dilatation, right ureteral dilatation associated with right VUR.
References: Department of Radiology, Children Emergency Hospital, Cluj-Napoca/RO.
Case 7: Six years old girl with bilateral urinary tract duplication and an associated left VUR (grade III).
Fig. 8
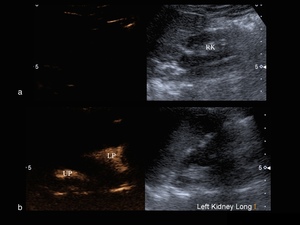
Fig. 8: Bilateral urinary tract duplication.
a) ce-VUS shows no reflux of contrast material in the right kidney (RK);
b) ce-VUS shows reflux of contrast material in the upper pole (UP) and in the lower pole (LP) of the left kidney.
References: Department of Radiology, Children Emergency Hospital, Cluj-Napoca/RO.
Case 8: Four months old girl with left urinary tract duplication and an associated left VUR (grade IV,
lower pole).
Fig. 9
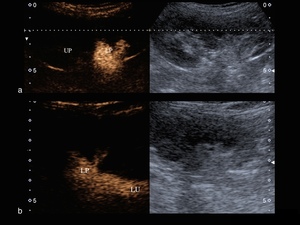
Fig. 9: Left urinary tract duplication.
a) ce-VUS (longitudinal scan) shows reflux of contrast material in the lower pole (LP) of the left kidney; b) ce-VUS shows reflux of contrast material in the LP of the left kidney and in the dilated left ureter (LU).
References: Department of Radiology, Children Emergency Hospital, Cluj-Napoca/RO.
Teaching points:
Reno-urinary abnormalities can be classified based on the following criteria:
- Number
- Position
- Dysplasia or hypoplasia
- Rotation and ascent
- Fusion
- Vessels
- Duplication
- Cystic disease
- Uretero-pelvic junction obstruction
Dysplasia/Hypoplasia represents a focal or diffuse structural alteration of the renal tissue with an increased parenchymal echogenicity and reduced corticomedullary differentiation.
It may be unilateral or bilateral and may associate severe obstructive uropathy and/or VUR 22.
Renal ectopia is an abnormal anatomical location of one or both of the kidneys,
which can frequently associate malrotation.
Most commonly,
the kidney is located in the pelvis; rarely it lies adjacent to the hemidiaphragm,
or even intra-thoracic when a Bochdalek hernia is associated 23.
Horseshoe kidney is a renal fusion abnormality (the lower poles are attached at the midline,
anterior to the aorta) and occurs in 1 in 600 individuals.
It can be associated with an impairment of urinary drainage and has a higher risk for being injured in abdominal trauma 22,
23.
Renal cysts can be congenital (genetic/non-genetic) or secondary (posttraumatic cysts,
postoperative cysts,
acquired cystic kidney disease in renal failure and after transplantation).
The non-genetic renal cysts include: cystic dysplasia,
multicystic dysplastic kidney,
medullary sponge kidney
,
localized cystic disease of the kidney,
simple cysts etc.
They are often associated with urinary tract obstruction or high-grade VUR 23,24.
Urinary tract duplication involves the presence of two separate pelvicalyceal collecting systems in one kidney and two draining ureters that insert into the bladder separately (complete duplication) or join above the bladder (partial duplication).
The ureter draining the upper pole of the kidney tends to insert in the bladder inferior and medial to the ureter draining the lower segment of the kidney.
Also,
the ureter draining the upper pole frequently ends in an ureterocele,
whereas the lower pole typically associates VUR 25,26.
Anomalies of the distal ureter:
Case 9: Three months old boy presented bilateral pelvicalyceal dilatation,
right ureteral dilatation and bilateral VUR (grade IV-right side,
grade II-left side).
The antero-posterior (AP) diameter of the right renal pelvis was 29mm and the AP diameter of the left renal pelvis 8.8mm.
Fig. 10
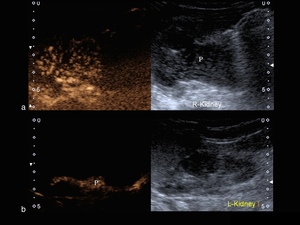
Fig. 10: Urinary tract dilatation.
a) ce-VUS shows right pelvicalyceal dilatation and right VUR;
b) ce-VUS shows left renal pelvis dilatation and left VUR.
References: Department of Radiology, Children Emergency Hospital, Cluj-Napoca/RO.
Case 10: Five months old boy presented bilateral pelvicalyceal dilatation,
bilateral dilated and tortuous ureters with an associated bilateral VUR (grade V).
Fig. 11
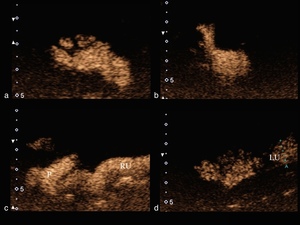
Fig. 11: Urinary tract dilatation.
a),b) ce-VUS (transverse scan of the kidneys) shows bilateral pelvicalyceal dilatation (a- RK; b-LK) and bilateral VUR;
c),d) ce-VUS (longitudinal scan) shows bilateral dilated ureters and bilateral reflux of contrast material (c-RU, d-LU).
References: Department of Radiology, Children Emergency Hospital, Cluj-Napoca/RO.
Case 11: Two months old boy with significant bilateral pelvicalyceal dilatation,
bilateral dilated ureters (the right ureter had a tortuous aspect) and bilateral VUR (grade V-right side,
grade IV-left side).
Fig. 12
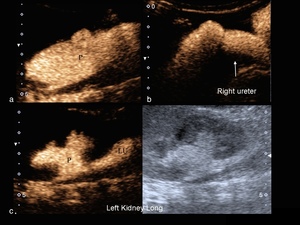
Fig. 12: Urinary tract dilatation.
a) ce-VUS shows right pelvicalyceal dilatation and right VUR;
b) ce-VUS shows right dilated and tortuous ureter associated with VUR;
c) ce-VUS (longitudinal scan) shows left pelvicalyceal dilatation and left dilated ureter associated with VUR.
References: Department of Radiology, Children Emergency Hospital, Cluj-Napoca/RO.
Case 12: One month old boy with an important left pelvicalyceal dilatation,
left dilated and tortuous ureter (3cm diameter),
associated with left VUR (grade V).
Fig. 13
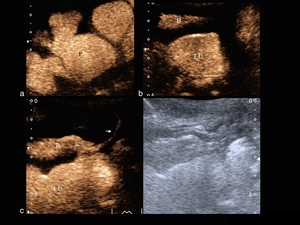
Fig. 13: Urinary tract dilatation. ce-VUS shows the presence of contrast agent in the left kidney (image a), bladder (B), left ureter (LU) and urethra (arrow). Image b) represents a transverse scan of the B and LU and image c) a longitudinal scan of the B, LU and urethra during voiding.
References: Department of Radiology, Children Emergency Hospital, Cluj-Napoca/RO.
Case 13: Two months old girl presented with the prenatal diagnosis of left ureterocele,
left urinary tract duplication and left renal dysplasia (pelvicalyceal dilatation of the upper pole).
Fig. 14
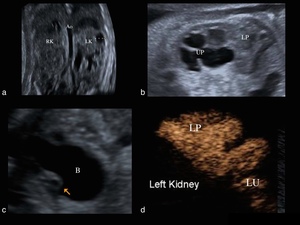
Fig. 14: Prenatal images (a, b, c). Pelvicalyceal dilatation of the left upper pole (UP), left ureterocele (arrow). ce-VUS shows left dilated and tortuous ureter associated with VUR (grade V - lower pole).
References: Department of Radiology, Children Emergency Hospital, Cluj-Napoca/RO.
Case 14: Three years old girl presented: bilateral urinary tract duplication,
bilateral atrophic upper pole,
significant bilateral pelvicalyceal dilatation,
left ureterocele and bilateral VUR (grade IV,
upper poles).
Fig. 15,
Fig. 16
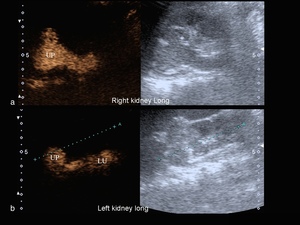
Fig. 15: Bilateral urinary tract duplication and left ureterocele. a), b) ce-VUS (longitudinal scan) shows the presence of contrast agent in both kidneys (upper poles).
References: Department of Radiology, Children Emergency Hospital, Cluj-Napoca/RO.
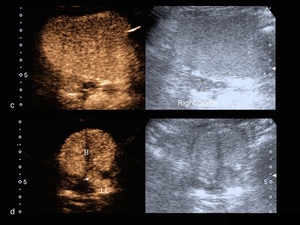
Fig. 16: ce-VUS shows the presence of contrast agent in both urinary tracts (RU, LU), bladder (B) and left ureterocele (arrow).
References: Department of Radiology, Children Emergency Hospital, Cluj-Napoca/RO.
Teaching points:
The normal diameter of the ureter in children is about 5mm.
An enlarged ureter may be primary or secondary,
refluxing or nonrefluxing,
obstructed or nonobstructed.
Primary dilated ureter is due to an idiopathic congenital alteration at the uretero-vesical junction,
while secondary dilated ureter is due to abnormalities involving the bladder or the urethra 26.
Ureterocele represent a cystic dilatation of the intravesical segment of the ureter.
It can be simple (the orifice is located in the bladder trigone) or ectopic (the orifice is located at the bladder neck or in the urethra),
3:1 ratio.
In 10% of cases it can be bilateral and is more frecvent in females than in males (4-7:1) 26.
Anomalies of the bladder:
Case 15: Seven years old boy presented a significant right pelvicalyceal dilatation,
bilateral Hutch diverticulum and right VUR (grade IV).
Fig. 17,
Fig. 18
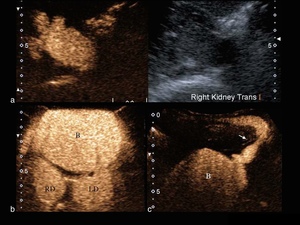
Fig. 17: Bilateral Hutch diverticulum (right diverticulum - RD, left diverticulum - LD) and right VUR.
a) Transverse scan of the right kidney shows pelvicalyceal dilatation and reflux of contrast agent;
b) Transverse scan of the bladder (B), RD and LD;
c) Transperineal scanning of the urethra during voiding (arrow) -normal findings.
References: Department of Radiology, Children Emergency Hospital, Cluj-Napoca/RO.
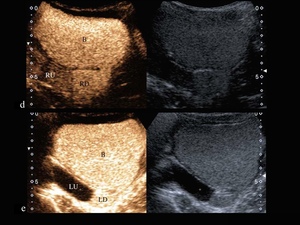
Fig. 18: d),e) ce-VUS shows the presence of contrast agent in the B, RD, LD and RU; there is no reflux in the LU.
References: Department of Radiology, Children Emergency Hospital, Cluj-Napoca/RO.
Teaching points:
Hutch diverticulum is a rare (2% of general population),
congenital bladder diverticulum located posteriorly and laterally to the ureteral orifice (near uretero-vesical junction) and can associate VUR (50% of cases).
Differential diagnosis includes: inverted ureterocele,
urachal diverticulum,
acquired diverticulum (neurogenic bladder,
posterior urethral valve) 25,27.
Anomalies of the urethra:
Case 16: One month old boy with significant bilateral pelvicalyceal dilatation,
posterior urethral valve and bilateral VUR (grade IV).
It was noticed a thickened bladder wall (7-8mm) and a large prostatic urethra (7mm).
Fig. 19
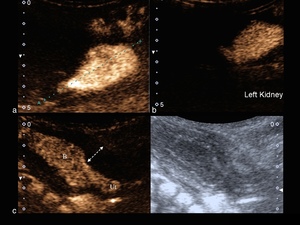
Fig. 19: Posterior urethral valve with a large posterior urethra (Ut) and a thickened bladder wall (arrow).
a), b) ce-VUS (longitudinal scan of the kidneys) shows bilateral pelvicalyceal dilatation (a- RK; b-LK) and bilateral VUR.
References: Department of Radiology, Children Emergency Hospital, Cluj-Napoca/RO.
Case 17: Seven days old boy with posterior urethral valve and multiple pseudodiverticula.
It was observed bilateral dilated and tortuous ureters associated with bilateral VUR (grade V).
Fig. 20
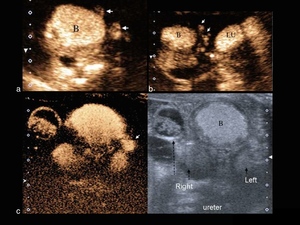
Fig. 20: Posterior urethral valve with multiple pseudodiverticula (white arrows). ce-VUS shows the presence of contrast agent in the bladder (B), in the multiple pseudodiverticula and in both dilated and tortuous ureters.
References: Department of Radiology, Children Emergency Hospital, Cluj-Napoca/RO.
Teaching points:
Posterior urethral valve is the most common congenital obstructive lesion of the urethra,
characterized by redundant folds of mucosa in its posterior wall.
It is more frequent in boys and associates secondary high-grade VUR or obstruction by thickened bladder wall and upper tract pathology (renal dysplasia,
dilatation of the collecting system) 22,23,26.

. ce-VUS shows bilateral VUR (microbubbles in the renal pelvis - P). References: Department of Radiology, Children Emergency Hospital, Cluj Napoca/RO.")
 Longitudinal scan of the right kidney shows the presence of microbubbles in the right renal pelvis (P) and also in the right ureter (RU);
b) Longitudinal scan of the bladder (B) shows reflux of contrast material in the RU.
References: Department of Radiology, Children Emergency Hospital, Cluj Napoca/RO.")
 Longitudinal scan - shows increased parenchymal echogenicity of the right kidney (RK) compared to the liver (L);
b) Transverse scan of the right kidney shows uroepithelial thickening (measured⇒2mm);
c) ce-VUS image shows right VUR (grade IV).
References: Department of Radiology, Children Emergency Hospital, Cluj Napoca/RO.")
 Transverse scan of the kidneys shows that the lower poles are attached in front of the aorta and the spine (Sp);
b) ce-VUS shows left VUR (grade II).
References: Department of Radiology, Children Emergency Hospital, Cluj-Napoca/RO.")
 Longitudinal scan of the right flank - shows the absence of the right kidney in the right renal fossa, between the liver (L) and the right psoas muscle (Pso); b) Longitudinal scan of the left kidney shows the presence of microbubbles in the renal pelvis. References: Department of Radiology, Children Emergency Hospital, Cluj-Napoca/RO.")
 Transverse scan of the urinary bladder (B) shows the right multicystic kidney (cyst = arrow) located posterior to it;
d) Transverse scan of the B shows reflux of contrast material in the left ureter. References: Department of Radiology, Children Emergency Hospital, Cluj-Napoca/RO.")
 Longitudinal scan of the right malrotated kidney - the renal pelvis (P) is located anteriorly;
b) ce-VUS shows a dilated left ureter (LU) with VUR;
c) ce-VUS shows right pelvicalyceal dilatation, right ureteral dilatation associated with right VUR. References: Department of Radiology, Children Emergency Hospital, Cluj-Napoca/RO.")
 ce-VUS shows no reflux of contrast material in the right kidney (RK);
b) ce-VUS shows reflux of contrast material in the upper pole (UP) and in the lower pole (LP) of the left kidney.
References: Department of Radiology, Children Emergency Hospital, Cluj-Napoca/RO.")
 ce-VUS (longitudinal scan) shows reflux of contrast material in the lower pole (LP) of the left kidney; b) ce-VUS shows reflux of contrast material in the LP of the left kidney and in the dilated left ureter (LU).
References: Department of Radiology, Children Emergency Hospital, Cluj-Napoca/RO.")
 ce-VUS shows right pelvicalyceal dilatation and right VUR;
b) ce-VUS shows left renal pelvis dilatation and left VUR.
References: Department of Radiology, Children Emergency Hospital, Cluj-Napoca/RO.")
,b) ce-VUS (transverse scan of the kidneys) shows bilateral pelvicalyceal dilatation (a- RK; b-LK) and bilateral VUR;
c),d) ce-VUS (longitudinal scan) shows bilateral dilated ureters and bilateral reflux of contrast material (c-RU, d-LU).
References: Department of Radiology, Children Emergency Hospital, Cluj-Napoca/RO.")
 ce-VUS shows right pelvicalyceal dilatation and right VUR;
b) ce-VUS shows right dilated and tortuous ureter associated with VUR;
c) ce-VUS (longitudinal scan) shows left pelvicalyceal dilatation and left dilated ureter associated with VUR.
References: Department of Radiology, Children Emergency Hospital, Cluj-Napoca/RO.")
, bladder (B), left ureter (LU) and urethra (arrow). Image b) represents a transverse scan of the B and LU and image c) a longitudinal scan of the B, LU and urethra during voiding.
References: Department of Radiology, Children Emergency Hospital, Cluj-Napoca/RO.")
. Pelvicalyceal dilatation of the left upper pole (UP), left ureterocele (arrow). ce-VUS shows left dilated and tortuous ureter associated with VUR (grade V - lower pole).
References: Department of Radiology, Children Emergency Hospital, Cluj-Napoca/RO.")
, b) ce-VUS (longitudinal scan) shows the presence of contrast agent in both kidneys (upper poles). References: Department of Radiology, Children Emergency Hospital, Cluj-Napoca/RO.")
, bladder (B) and left ureterocele (arrow). References: Department of Radiology, Children Emergency Hospital, Cluj-Napoca/RO.")
 and right VUR.
a) Transverse scan of the right kidney shows pelvicalyceal dilatation and reflux of contrast agent;
b) Transverse scan of the bladder (B), RD and LD;
c) Transperineal scanning of the urethra during voiding (arrow) -normal findings.
References: Department of Radiology, Children Emergency Hospital, Cluj-Napoca/RO.")
,e) ce-VUS shows the presence of contrast agent in the B, RD, LD and RU; there is no reflux in the LU.
References: Department of Radiology, Children Emergency Hospital, Cluj-Napoca/RO.")
 and a thickened bladder wall (arrow).
a), b) ce-VUS (longitudinal scan of the kidneys) shows bilateral pelvicalyceal dilatation (a- RK; b-LK) and bilateral VUR.
References: Department of Radiology, Children Emergency Hospital, Cluj-Napoca/RO.")
. ce-VUS shows the presence of contrast agent in the bladder (B), in the multiple pseudodiverticula and in both dilated and tortuous ureters.
References: Department of Radiology, Children Emergency Hospital, Cluj-Napoca/RO.")