Intussusception may occur in any gastrointestinal segment and the imaging findings are similar regardless the location.
The most commonly used imaging methods are ultrasound and CT.
Ultrasound
In children,
ultrasound is the modality of choice,
as it has both high sensitivity and specificity,
and it is fast,
non-invasive and easy to perform.
However,
in the adult population there may be false positives due to bowel thickening secondary to conditions such as lymphoma or an inflammatory mass.
False negative results may occur if there is abundant overlying bowel.
Classic findings include a “target sign” or “doughnut sign” on transverse scans,
consisting of alternating hyperechoic and hypoechoic concentric rings that represent alternating layers of mucosa,
bowel wall,
and mesenteric fat.
On longitudinal scans there is the “pseudokidney sign”,
with multiple thin parallel stripes of varying degrees of echogenicity with a sandwich-like appearance.
Nevertheless CT is mandatory in this age group to confirm the diagnosis,
to determine the underlying cause,
to find a lead point and to evaluate complications.
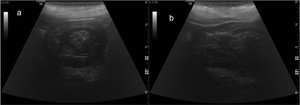
Fig. 1: Gastric intussusception on a 91 year old female with vomiting and hypotension. (a) US scan shows the “target sign” on transverse scan with alternating hyperechoic and hypoechoic concentric rings; b) US scan demonstrates the “pseudokidney sign” on the longitudinal plane, with a central hyperechoic region surrounded by a hypoechoic ring.
Computer Tommography
Computed tomography is the most useful imaging modlity in the adult population in both making the diagnosis and assessing for an associated lead point.
The imaging findings depend on the severity and duration of the intussusception,
as well as on the presence of a lead point,
the configuration of the lead mass,
the degree of bowel wall edema and the amount of invaginated mesenteric fat.
The earliest finding is of a “target” appearance,
when the beam is perpendicular to the longitudinal axis of the intussusception.

Fig. 2: 32 year old male patient with ulcerous colitis. (a) Coronal contrast-enhanced CT image shows the “target” appearance. (b) Axial contrast-enhanced CT image demonstrates an ileoileal intussusception, without proximal bowel distension.
Later a sausage-shaped mass with different layers of attenuation develops when the CT beam is parallel to its longitudinal axis,
representing mesenteric fat and bowel wall.
Lastly,
a reniform mass develops due to edema,
mural thickening and vascular compromise.
Additional findings include small bowel obstruction,
with fluid levels and proximal bowel distension,
and there may be traction of the mesenteric arcade as it becomes involved in the intussusception.
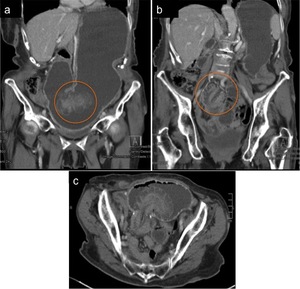
Fig. 3: 78 year old female patient with abdominal pain and vomiting. The patient had been previously submited to a Billroth type II surgery due to peptic ulcer disease. (a) and (b) Coronal contrast-enhanced CT images show gastric distention and an intussusception, with marked mural thickening and edema. (c) Axial contrast-enhanced CT image demonstrates the intussusception of the afferent limb, with evident mural thickening and edema.
While the appearance of intussusception is characteristic on CT,
its etiology cannot usually be established,
with the exceptions of lipoma,
a long intestinal tube and a known abdominal metastatic disease.
It has been reported that intussusceptions with a neoplastic lead point are longer and have a significantly larger diameter than non-neoplastic ones.
Moreover proximal dilatation of small bowel appears to be significantly more common in intussusceptions with a neoplastic lead point
Intussusception according to location
Gastric Intussusception
Foregut intussusception is rare and it is more commonly caused by intussusception of the gastric remnant through a gastrojejunal anastomosis or of gastric polyps through the pylorus into the duodenum.
Possible lead points include adenoma,
leiomyoma,
lipoma,
hamartoma,
inflammatory fibrinoid polyp,
adenocarcinoma and leiomyosarcoma.
Typical findings include foreshortening and narrowing of the gastric antrum,
converging of mucosal folds in the antrum or duodenum,
prepyloric collar-shaped outpouchings,
and widening of the pyloric canal and the duodenum with an associated lead point.
Fig. 1: Gastric intussusception on a 91 year old female with vomiting and hypotension. (a) US scan shows the “target sign” on transverse scan with alternating hyperechoic and hypoechoic concentric rings; b) US scan demonstrates the “pseudokidney sign” on the longitudinal plane, with a central hyperechoic region surrounded by a hypoechoic ring.

Fig. 4: 91 year old female with vomiting and hypotension. Axial contrast-enhanced CT image demonstrates an instussusception involving the transition from the gastic fundus to the body, with some mural thickening and edema. There is no proximal gastric distension.

Fig. 5: 72 year old male patient with nausea and vomiting. (a) Axial contrast-enhanced CT image shows an intussusception through the pylorus into the duodenum. (b) Coronal contrast-enhanced CT image demonstrates the same intussusception, highlighting mucosal edema.
The patient was submited to an atypical gastrectomy and the pathologic examination revealed a gastrointestinal stromal tumor.
Small Bowel Intussusception
Small-bowel intussusceptions are more commonly due to benign lesions and include gastrointestinal stromal tumors (GISTs),
nonneoplastic polyps,
congenital lesions such as Meckel’s diverticulum and intestinal duplication,
inflammatory lesions and trauma.
Malignant lesions are responsible for 15% of cases,
most often metastasis from melanoma.
Idiopathic intussusceptions account for approximately 20% of the situations.
It is reported that small bowel intusssuception without a lead point is more common than intussusception with a lead point and it appears as a nonobstructing segment,
usually smaller in diameter and shorter than an intussusception with a lead point.
Duodenojejunal intussusception is rare due to fixation of a large portion of the duodenum,
preventing telescoping of that segment of the bowel.
CT can show an elongated duodenum with or without the characteristic target-like lesion in the proximal jejunum,
accompanied by dislocation of the ampulla of Vater.
Transient intussusception is more common in the proximal small bowel,
where the peristaltic activity is normally greater.
Surgical intervention is considered necessary in intussusception when the patient is symptomatic.
When the patient is asymptomatic and the intussusceptions most likely transient,
no therapeutic is needed.
Fig. 2: 32 year old male patient with ulcerous colitis. (a) Coronal contrast-enhanced CT image shows the “target” appearance. (b) Axial contrast-enhanced CT image demonstrates an ileoileal intussusception, without proximal bowel distension.
Large Bowel Intussusception
More than half of large-bowel intussusceptions are associated with malignant lesions,
not only primary (adenocarcinoma and lymphoma) but also metastatic disease,
reflecting the greater prevalence of malignant tumors in the colon compared with the small bowel.
Approximately 30% the situations are caused by a benign lesion and include lipomas,
GISTs,
polyps,
endometriosis,
previous anastomosis… Idiopathic intussusception accounts for approximately 10% of the cases.
It has also been reported in diseases that predispose to bowel wall hemorrhage or edema such as Henoch-Schönlein purpura,
leukemia,
anticoagulant therapy,
chronic renal failure,
and due to antibiotic therapy for pseudomembranous colitis with Clostridium difficile.
Intussusception following abdominal surgery may be related to a variety of predisposing factors,
including intestinal anastomotic suture lines,
adhesions,
submucosal bowel oedema,
intestinal dysmotility and electrolyte imbalance.
Intussusception involving the sigmoid or rectum is very rare.

Fig. 6: Asymptomatic 39 year old female patient. Coronal (a) and axial (b) contrast-enhanced CT images show a colocolic intussusception near the hepatic flexure.

Fig. 7: 86 year old male patient with diarrhea, vomiting and anemia. (a) and (b) Axial contrast-enhanced CT images show signs of an intussusception through the sigmoid to the rectum. Pathology revealed a rectal adenocarcinoma.
