1) 7 different CT protocols identified for acute GI bleed cases. 74% cases were done as per recommended protocols ie Triple phase CT (plain,
arterial,
portal venous phase).
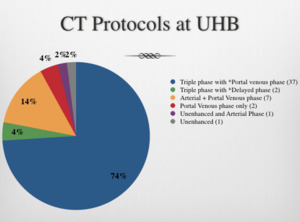
Table 1: Variable CT protocols for acute GI bleed.
2) Of the 50 cases,
14% were initially reported as positive for GI bleeding,
of which 6% (3 cases) were later discovered to be false positive,
on second review.
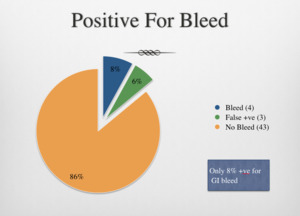
Table 2: Incidence of GI bleed in our cohort.
3) 2 false positive cases for learning purpose.
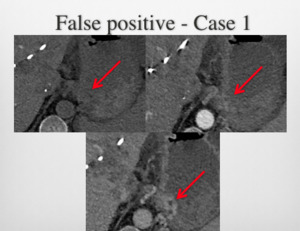
Fig. 1: False Positive Case 1: High attenuating foci on arterial and portal venous phase images near the gastro-oesophageal junction misinterpreted by the on call registrar as GI Bleed. However, these changes which also present on a recent CT, were accurately reported as varices (not active bleeding point) by the supervising consultant and an appropriate addendum added. Pt did not have any further intervention.
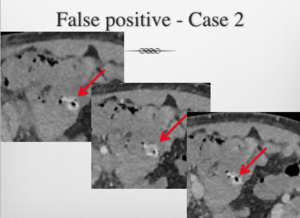
Fig. 2: False Positive Case 2: High attenuating intraluminal material on pre-contrast images unchanged on the post contrast sequences, misinterpreted as acute GI Bleed initially by the on call radiology registrar. However, the supervising consultant made the correct interpretation subsequently as no active haemorrhage. An appropriate addendum was added to the initial report and no further intervention needed (as history did not suggest an active GI Bleed - Persistant Hb dropping despite blood products - blood soaked abdominal dressings over open abdomen. Question: ? sepsis related bleeding wound edge/intra abdominal bleeding point)
4) 72% of cases presented as Upper GI bleed,
22% as lower GI bleed,
6% uncertain source.
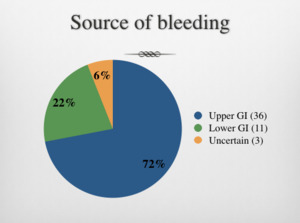
Table 3: Source of GI bleed based on the clinical presentation.
5) 77% of upper GI bleed cases had OGD as per the local guidelines.
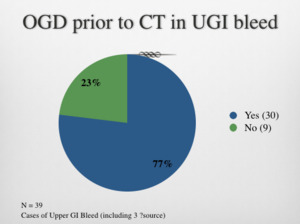
Table 4: OGD investigation prior to CT study for suspected Upper GI bleed cases.
6) After initial CT,
4% had emergency laparotomy,
28% had radiological intervention, 68% cases were managed conservatively.
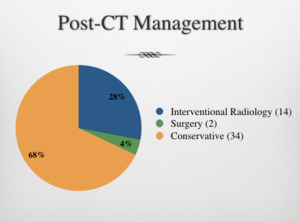
Table 5: Management after initial CT (excludes the false +ve cases, as IR not deemed necessary).
14 IR patients – Only 2 were CT+ve cases. IR showed bleed in 1 of these cases.
- 6 were found to have bleed and embolised, previously CT-ve cases.
– 4 had empirical embolisation in the absence of bleed on-table catheter angiogram.
2 surgery patients - 1 had perforated DU (Survived), 1 had bleeding rectal ulcers (Died due to septic shock)
14 conservatively managed patients did not have any evidence of active or ongoing GI Bleed.
7) 2 cases of active GI bleed with subsequent radiological intervention.
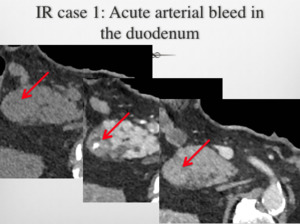
Fig. 3: IR case 1 CT images: Acute duodenal bleed, treated by GDA and side branch embolisation.
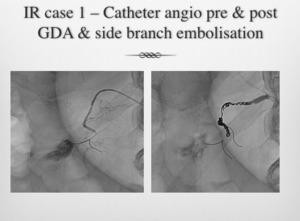
Fig. 4: IR case 1 Angiogaphy images: Acute duodenal bleed, treated by GDA and side branch embolisation.
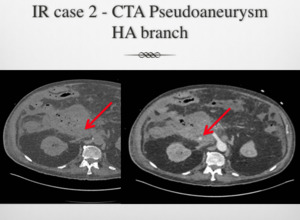
Fig. 5: IR Case 2 CT images: Hepatic artery bleed and pseudoaneurysm, embolised.
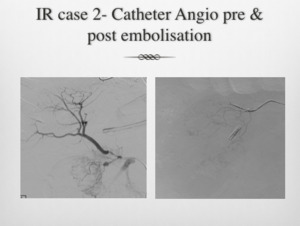
Fig. 6: IR Case 2 Angiography images: Hepatic artery bleed and pseudoaneurysm, embolised.
