Type:
Educational Exhibit
Keywords:
Ultrasound, Mammography, CT, Breast, Biopsy, Surgery, Cancer, Cysts, Abscess
Authors:
H. W. Yoo, S. Y. Kim, S. Huh; Cheonan/KR
DOI:
10.1594/ecr2018/C-1351
Findings and procedure details
Benign male breast disease
Gynecomastia
- Most common breast disease in men
- Nonneoplastic hyperplasia of the ductal and stromal elements of malbe breast in resoponse to hormonal stinulation
- Causes
- Estrogen effects : Neonates,
adolescents and the elderly
- Endocrine and hormonal disorders : Klinefelter's syndrome,
neoplasms,
drug use,
systemic disease,
obesity and medication use
- Clinical manifestations
- A palpable abnormlaity,
focal breast tenderness,
or a subjective
burning senssation
- Unilateral or bilateral
- Usually subareolar in location
- Three patterns,
based on the mammography findings.
- Nodular
▷ Well defined nodule or triangular shape nodule in subareolar
area
▷ The patients with symptoms of less than 1 year duration
- Dendritic(Fig.2)
Fig. 2: Dendritic gynecomastia in 70 years-old man
A. Left MLO view shows retroareolar soft tissue density with prominent extensions that radiate into the deeper adipose tissue
B. Ultrasonography shows ill-defined hypoechoic mass with spiculated margins without posterior acoustic shadowing(arrows).
▷ Finger like projections extending into the retroareolar breast
tissue
▷ The patients whose symptoms persist for more than 1 year
- Diffuse (Fig.
3)

Fig. 3: Diffuse gynecomastia in 61 years-old man.
A. Right MLO view shows diffusely ill-defined hyperdensity that is similar to heterogenous dense female breast(arrows).
B. Ultrasonography shows diffuse normal glandular tissue that colsely resemble female breast(open arrow).
▷ It may appear similar to a heterogenously dense female
breast without a mass or lymphadenopathy
▷ Often associated with exposure to exogenous estrogen
- Distinguishing with breast cancer
- Breast cancer
▷ Usually unilateral (Bilateral : About 1.4%)
▷ Eccentric location from the nipple
▷ Secondary signs
: Nipple retraction,
skin thickening,
increased breast
trabeculation,
axillary lymphadenopathy
- Gynecomastia
▷ Usually bilateral
▷ Subareolar location
▷ Ill-definted margin
▷ No secondary signs
▷ USG : Parallel growth pattern,
Lack of posterior acoustic
enhancement,
variable vascularity
Pseudogynecomastia (Fig.
4)

Fig. 4: Pseudogynecomastia in 61 years-old man
A,B. Left MLO view and ultrasonography show rich fatty tissue without glandular tissue
- Clinically similar to gynecomastia
- Fatty tissue proliferation without glandular tissue
Myofibroblastoma(Fig.
5)
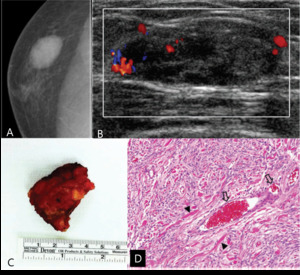
Fig. 5: Myofibroblastoma in 52-years old man
A. Right craniocaudal (CC) view shows circumscribed oval hyperdense mass in outer breast
B. Color Doppler ultrasonography shows circumscribed oval hypoechoic mass in right upper outer breast with increased vascularity within the mass
C. Specimen shows about 2.2cm sized and well-defined mass without adhesion to pectoralis muscle.
D. Histopathology shows spindle cells(arrowheads) with mild proliferation of vascular structures (Open arrows) without atypia nor mitosis(H & E, ×100).
- Rare benign stromal tumor
- Occurs in men in the 6th to 7th decades of life.
- Clinically as a slow growing,
unilateral,
painless,
mobile mass that has been present for a along time
- Mammographic features
- a well-defined,
round to ovoid,
dense mass
- US
- a solid,
well-circumscribed homogenously hypoechoic mass
- Less commonly,
ill-defined appearance with posterior shadowing
- MRI
- Heterogenous enhancement similar to that seen in fibroadenoma
- With nonenhancing internal septations on T2WI
Phyllodes tumor
- Rare and mainly observed in middle-aged women
- Widely varying mean age of from 30 to 52 years in the literature.
- Arise from stromal component
- Characterized by double-layered epithelial component arranged in clefts surrounded by a hypercellular mesenchymal component that is typically organized in a left-like pattern
- Classified into benign,
borderline and malignant category
- Benign
: 0-4 mitoses/10 hpf,
pushing margins,
and minimal or moderate stromal overgrowth with minimal stromal cellularity and atypia
- Borderline or low-grade maligant phyllodes tumor
: 5-9 mitoses/10 hpf,
pushing or infiltrating margins,
moderate stromal cellularity and atypia,
with overgrowth
- Malignant or high-grade phyllodes tumor
: >10 mitoses/10 hpf,
infiltrating margins,
moderate to marked stromal cellularity,
and atypia,
with overgrowth.
- Mammography (Fig.
6)
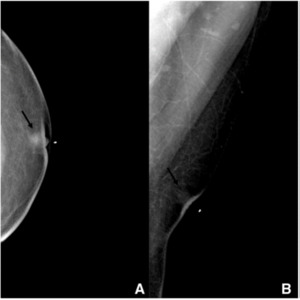
Fig. 6: Borderline phyllodes tumor in 39-year-old man
A. Craniocaudal and B. Mediolateral oblique mammogram shows a 1cm sized circumscribed oval mass with equal density on the subareolar area of the left breast (arrow) with skin thickening and nipple retraction. There were no associated calcification.
- Well-defined margins than ill-defined margins
- USG(Fig.
7)
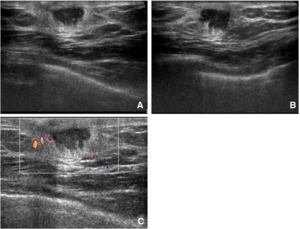
Fig. 7: Borderline phyllodes tumor in 39-year-old man
A,B,C. Transverse, longitudinal, and color doppler USG reveals a 1.5-cm-sized indistinct oval heterogenously echoic mass with mild edema, but with no vascularity.
- Borderline and malignant phyllodes tumors are observed as well-defined oval lobulated masses with posterior enhancement,
like in benign phyllodes tumors.
- The rapidly increasing size results in prominent veins around the tumor as well as increased vascularity on color doppler image
- Calcification can be found but infrequent and not associated with malignancy.
- There is no report that showed statistically significant imaging differences between maligant and benign phyllodes tumors based on mammography and USG
Inflammed granulation tissue(Fig.
8)
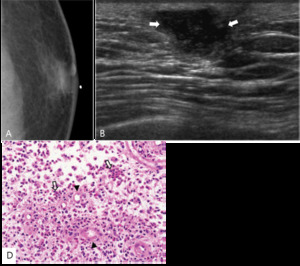
Fig. 8: Inflammed granulation tissue in 51-years-old man.
A. Left CC view shows glandular density just underneath a radiopaque skin marker attached at palpable site.
B. Ultrasonography shows partly angulated oval complex cystic nodule in left subareolar area (arrows).
C. Histopathology shows granulation tissue which consits of fibrosis, vessels(arrowheads), and multiple inflammatory cells(open arrows).
- Granulation tissue
- A young connective tissue that is rich in capillaries and continues to proliferate vigorously.
- Can be observed at restoration of wound defect,
organization of foreign body,
chronic inflammation or reactive inflammation of interstitial material accompanied by tumor proliferation
Tuberculosis mastitis(Fig.
9)
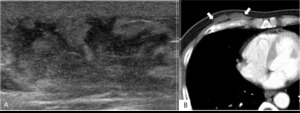
Fig. 9: Tuberculosis mastitis in 51-years-old man.
A. Ultrasonography shows ill-defined oval heterogenous hypoechoic mass with skin thickening.
B. CT shows well-defined lobulated nonenhancing hypodense mass in subcutaneous fatty layer (arrows).
-
Route of spreading to the breast : Hematogenic,
lymphatic,
direct extension from the thoracic wall or the axillary lymph nodes(Most common),
or by inoculation through traumatized skin or ducts.
-
Difference between nontuberculous mastitis
- Extension of chest wall or pleural space abscess beyond the capsule of breast through the fistula
-
Pathologic classification : Nodular,
disseminated,
sclerosing form
-
Mammography
- Nonspecific findings : Normal or diffuse increased opacity
- Well-defined nodule : nodular form or cold abscess form
-
- Rarely can see the band-like appearance due to fistula between abscess and skin.
- USG
- Cold abscess form : Well-defined hypoechoic lesion without acute inflammation
- Nodular form : Ill-defined hyperechoic lesion,
similar to that of nontuberculous mastitis
→ Clinically accompanied acute inflammatory signs are helpful for differential diagnosis.
Subareolar abscess(Fig.
10)

Fig. 10: Subareolar abscess in 56-years-old man.
Ultrasonography shows partly microlobulated relatively round complex cystic mass in left subareolar area. Overlying skin thickening is also seen.
- Chronic lesion associated with duct ectasia
- Tend to recur,
if it does not resected.
- Nipple edema,
nipple discharge.
- Mammography : Ill-defined subareolar mass with thickening of fibrous trabecula.
- USG : Incomplete focal mass with fluid collection.
Malignant male breast disease
Ductal carcinoma in situ(DCIS) and invasive ductal carcinoma(IDC)
- IDC(Fig.
11,
12)
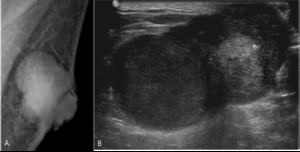
Fig. 11: Invasive ductal carcinoma in 73-years-old man
A. Left MLO view shows circumscribed lobular hyperdense mass with adjacent skin thickening in subareolar area
B. Ultrasonography shows partly microlobulated and circumscribed oval heterogenous hypoechoic mass

Fig. 12: Invasive ductal carcinoma in 73-years-old man
A. Ultrasonography shows microlobulated oval heterogenous hypoechoic mass with compression of pectoralis major muscle.
B. CT shows well-defined lobulated heterogenous enhancing mass with central necrosis
C. PET-CT shows high FDG-uptake (maxSUV 7.9) in the left breast mass.
- 85% of male breast cancer.
- Associated DCIS : 35~50% of patients
- Mammography
: Well-defined irregular hyperdense subareolar mass
- Microcalcification
: rare, more coarse and fewer number compared to female.
- USG
: nonparallel pattern hypoechoic mass,
microlobulated or
spiculated margin
: Microcalcification → dot-like hyperechogenecity
: Posterior acoustic pattern is not helpful for distinguishing
between benign and malignant tumor
- DCIS(Fig.
13)
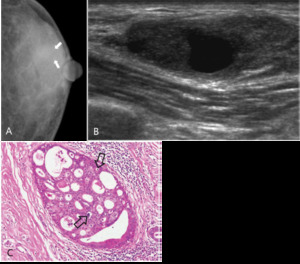
Fig. 13: Ductal carcinoma in situ in 51-years-old man.
A. Left CC view shows diffuse gynecomastia without definitely delineated mass. Combined benign calcifications (arrows) are seen in outer breast.
B. Ultrasonography shows circumscribed oval complex cystic nodule in upper outer breast
C. Histopathology shows cribriform shaped ductal dilatation. Intraluminal calcifications (open arrows) are also seen in some of the dilated duct.
Ductal carcinoma in situ(cribriform type) was confirmed by excisional biopsy (H & E, ×100)
- About 5-10% of male breast cancer
(Very low compared to female)
Mucinous carcinoma(Fig.
14)
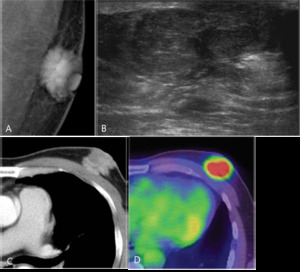
Fig. 14: Mucinous carcinoma in 53-years-old man.
A. Left MLO view shows spiculated irregular hyperdense mass in subareolar area.
B. Ultrasonography shows circumscribed oval heterogenously isoechoic mass.
C. CT shows lobulated hterogenous enhancing mass in subareolar area of left breast
D. PET-CT shows hypermetabolism(maxSUV 5.3) within the left subareolar mass.
- Rare male breast cancer (Less than 2% of male breast cancer)
- Associated metastatic lymph node : 2-4%(Lower than IDC)
- Better prognosis compared to IDC
- Mammography
- Well-defined round mass with iso or hypodensity
- Can be misdiagnosis as benign tumor
- Ill-circumscribed margin can be seen in most of case when performing spot compression
- USG
- Well-circumscribed mass showing the same echo as the surrounding fat.

.")
.
B. Ultrasonography shows diffuse normal glandular tissue that colsely resemble female breast(open arrow).")

 view shows circumscribed oval hyperdense mass in outer breast
B. Color Doppler ultrasonography shows circumscribed oval hypoechoic mass in right upper outer breast with increased vascularity within the mass
C. Specimen shows about 2.2cm sized and well-defined mass without adhesion to pectoralis muscle.
D. Histopathology shows spindle cells(arrowheads) with mild proliferation of vascular structures (Open arrows) without atypia nor mitosis(H & E, ×100).")
 with skin thickening and nipple retraction. There were no associated calcification.")

.
C. Histopathology shows granulation tissue which consits of fibrosis, vessels(arrowheads), and multiple inflammatory cells(open arrows).")
.")


 in the left breast mass.")
 are seen in outer breast.
B. Ultrasonography shows circumscribed oval complex cystic nodule in upper outer breast
C. Histopathology shows cribriform shaped ductal dilatation. Intraluminal calcifications (open arrows) are also seen in some of the dilated duct.
Ductal carcinoma in situ(cribriform type) was confirmed by excisional biopsy (H & E, ×100)")
 within the left subareolar mass.")